











Obsessive-Compulsive Disorder (OCD) – Sign and Symptoms, Risk Factors, Complications, Diagnosis, Treatment and Prevention
Obsessive-Compulsive Disorder (OCD) is a chronic, often debilitating neuropsychiatric condition defined by the presence of persistent obsessions, compulsions, or both, causing significant distress and functional impairment. It is classified in the DSM-5 under "Obsessive-Compulsive and Related Disorders," a category that also includes body dysmorphic disorder, hoarding disorder, and trichotillomania, reflecting shared neurobiological and phenomenological features. OCD affects approximately 1–3% of the global population across all demographics, with an estimated worldwide prevalence of over 70 million individuals. The condition carries a substantial burden of disease: the World Health Organization (WHO) has ranked OCD among the top ten causes of disability worldwide. Its onset typically occurs in late childhood, adolescence, or early adulthood, with a bimodal distribution peaking in males during childhood (ages 6–15) and in females during early adulthood (ages 20–29). A slight female predominance is observed in adult populations.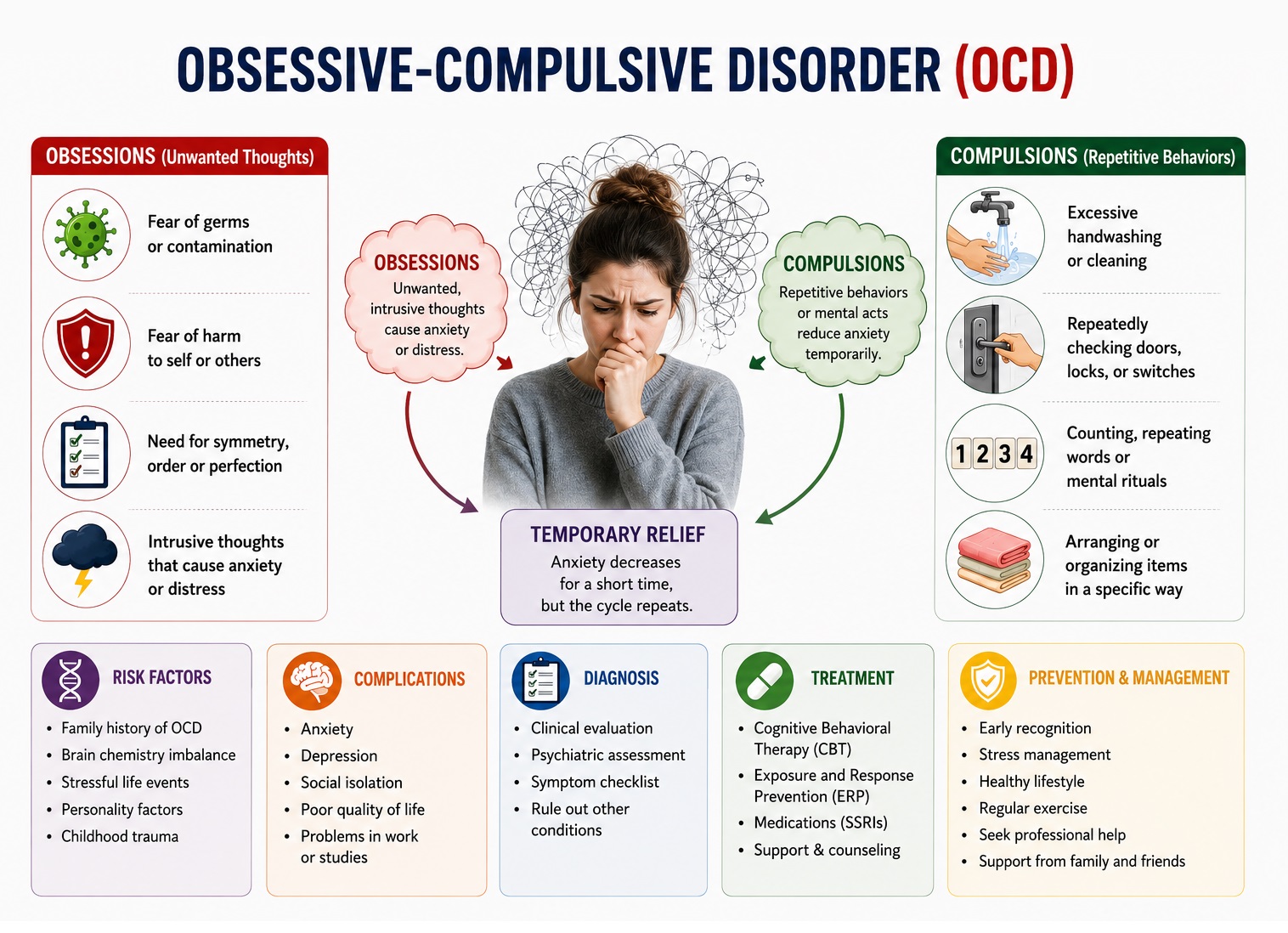 The etiology of OCD is multifactorial, involving the interplay of genetic susceptibility, neurobiological dysregulation, and environmental triggers. Despite its prevalence and severity, OCD remains significantly underdiagnosed, with an average delay of 14–17 years between symptom onset and initiation of appropriate treatment — a gap that underscores the critical need for clinical awareness.
The etiology of OCD is multifactorial, involving the interplay of genetic susceptibility, neurobiological dysregulation, and environmental triggers. Despite its prevalence and severity, OCD remains significantly underdiagnosed, with an average delay of 14–17 years between symptom onset and initiation of appropriate treatment — a gap that underscores the critical need for clinical awareness.
Pathophysiology of OCD
Neurobiological Mechanisms
The neurobiological model of OCD centers on dysfunction within the cortico-striato-thalamo-cortical (CSTC) circuits — a series of parallel loops connecting the prefrontal cortex to the striatum, globus pallidus, and thalamus, before projecting back to cortical areas.
Three key circuit dysfunctions have been identified:
- Orbitofrontal cortex (OFC)–caudate nucleus loop: Hyperactivity in this loop is thought to generate intrusive, repetitive thoughts. Neuroimaging studies consistently demonstrate increased metabolic activity in the OFC and caudate nucleus in patients with OCD, activity that normalizes following successful treatment.
- Anterior cingulate cortex (ACC): The ACC is involved in error detection and conflict monitoring. Hyperactivation leads to an exaggerated sense that "something is wrong," driving the compulsive need to correct perceived errors — a phenomenon sometimes referred to as an "error signal" that fails to extinguish.
- Basal ganglia: Abnormal filtering within the basal ganglia results in failure to gate irrelevant stimuli, allowing intrusive thoughts to reach conscious awareness repeatedly.
Neurotransmitter Dysregulation
Serotonin dysregulation has long been implicated in OCD, supported by the efficacy of selective serotonin reuptake inhibitors (SSRIs) as first-line pharmacotherapy. However, the precise role of serotonin remains complex; it is likely a modulator rather than a direct cause. Dopaminergic dysfunction — particularly within mesocortical and mesolimbic pathways — also contributes, explaining why dopamine-modulating agents (e.g., low-dose antipsychotics) augment SSRI response in treatment-resistant cases. Emerging evidence also implicates glutamatergic dysregulation, with elevated glutamate levels found in the caudate nucleus of OCD patients.
Genetic Architecture
OCD is moderately heritable, with twin studies estimating heritability at 40–65%. First-degree relatives of individuals with OCD have a 4–8 times greater risk of developing the disorder. Candidate genes include those encoding the serotonin transporter (SLC6A4), dopamine receptors (DRD4), and glutamate transporter (SLC1A1). OCD exhibits significant genetic overlap with Tourette syndrome and other tic disorders, reinforcing the concept of a neuropsychiatric spectrum.
Signs and Symptoms of OCD
Clinical Framework: Obsessions and Compulsions
Obsessions are recurrent, persistent, and intrusive thoughts, urges, or images that cause marked anxiety or distress. They are ego-dystonic — experienced as foreign, unwanted, and inconsistent with the individual's values — distinguishing them from the ego-syntonic ruminations seen in depression or the overvalued ideas of psychotic disorders.
Compulsions are repetitive behaviors (e.g., hand washing, ordering, checking) or mental acts (e.g., counting, praying, silently repeating words) that a person feels driven to perform in response to an obsession, or according to rules that must be applied rigidly. Compulsions are performed with the aim of reducing distress or preventing a feared outcome, though the relief is invariably temporary.
To meet DSM-5 diagnostic criteria, obsessions and/or compulsions must be time-consuming (more than one hour per day) or cause significant distress or functional impairment.
Common Symptom Dimensions
OCD is phenomenologically heterogeneous, but symptom clustering research has identified several well-validated dimensions:
| Dimension | Obsessional Content | Typical Compulsions |
|---|---|---|
| Contamination | Fear of germs, illness, or spreading harm | Excessive washing, cleaning, avoidance |
| Symmetry/Ordering | Need for exactness, "just right" feelings | Arranging, repeating, counting |
| Forbidden/Taboo Thoughts | Aggressive, sexual, or religious intrusions | Mental neutralization, reassurance-seeking |
| Harm/Checking | Fear of causing harm through negligence | Repeated checking (locks, appliances, doors) |
| Hoarding | Fear of losing important items | Inability to discard possessions |
Prodromal and Early Phase
The early presentation of OCD may be subtle. Clinicians should recognize:
- Mild, intermittent intrusive thoughts that the patient dismisses or attempts to suppress
- Emerging avoidance behaviors to circumvent anxiety-triggering stimuli
- Excessive doubt or indecisiveness in daily tasks
- Emerging ritualistic routines with minor distress tolerance
Acute and Established Phase
As the disorder progresses, the clinical picture becomes more overt:
- Time-consuming rituals (often exceeding several hours daily)
- Significant interference with occupational, academic, and social functioning
- Secondary anxiety, shame, and concealment
- Family accommodation behaviors (relatives participating in or enabling rituals)
Severe and Late Presentations
In severe, longstanding OCD:
- Rituals may occupy the majority of waking hours
- Complete social withdrawal and inability to maintain employment
- Severe comorbid depression, often with passive suicidal ideation
- "OCD insight" may diminish — some patients hold their beliefs with overvalued conviction (poor insight OCD) or near-delusional intensity, which the DSM-5 specifies as distinct subtypes
Neuropsychological Features
- Cognitive inflexibility: Difficulty shifting mental set, perseveration
- Impaired response inhibition: Reduced ability to suppress intrusive thoughts or halt compulsive urges
- Deficits in non-verbal memory and visuospatial function
- Heightened threat appraisal: Overestimation of threat and inflated sense of personal responsibility
Risk Factors of OCD
Genetic and Biological Factors
A positive family history of OCD or related disorders (e.g., Tourette syndrome, trichotillomania, body dysmorphic disorder) is the most consistently replicated risk factor. Neurobiological vulnerabilities — including temperamental anxiety sensitivity and reward processing abnormalities — also confer risk.
Neurological Conditions
OCD symptoms may arise secondary to neurological conditions affecting basal ganglia function, including Huntington's disease, Sydenham's chorea, and Parkinson's disease. The PANDAS (Pediatric Autoimmune Neuropsychiatric Disorders Associated with Streptococcal infections) hypothesis proposes that group A streptococcal infection can trigger acute-onset OCD in susceptible children via autoimmune mechanisms, though this remains an area of ongoing research.
Environmental and Psychosocial Factors
- Childhood physical, sexual, or emotional abuse
- Adverse life events and chronic psychosocial stress
- Perinatal complications (premature birth, hypoxic events)
- Reinforcement of compulsive behaviors through family accommodation
- Social learning from a parent or caregiver modeling OCD-like behaviors
Psychological Factors
Cognitive models highlight the role of dysfunctional beliefs, including:
- Inflated responsibility: Believing one can and must prevent harm
- Overimportance of thoughts: Believing that having a thought makes it more likely to occur or morally equivalent to an action (thought-action fusion)
- Intolerance of uncertainty: Extreme discomfort with ambiguous situations
- Perfectionism: Belief that imperfect performance leads to catastrophic consequences
Diagnosis of OCD
Diagnostic Criteria (DSM-5) of OCD
OCD is diagnosed when:
- Obsessions, compulsions, or both are present
- These are time-consuming (>1 hour/day) or cause clinically significant distress or functional impairment
- The symptoms are not attributable to a substance or medical condition
- The disturbance is not better explained by another mental disorder
The clinician should specify insight level (good/fair, poor, or absent/delusional) and presence of a tic-related specifier, which has treatment implications.
Clinical Assessment
History taking should comprehensively explore:
- Onset and duration of symptoms
- Full range of obsessive and compulsive symptom domains
- Impact on daily functioning, relationships, and occupation
- Degree of insight and resistance to compulsions
- Family accommodation behaviors
- Personal and family psychiatric history
- Current medications and medical conditions
Standardized assessment instruments recommended in clinical practice include:
- Yale-Brown Obsessive Compulsive Scale (Y-BOCS): The gold-standard clinician-administered scale measuring severity of obsessions and compulsions independently. A score of 16–23 indicates moderate OCD; ≥24 indicates severe OCD.
- Obsessive-Compulsive Inventory–Revised (OCI-R): A validated self-report measure useful for initial screening and monitoring treatment response.
- Children's Y-BOCS (CY-BOCS): Modified version for pediatric populations.
Differential Diagnosis of OCD
Accurate diagnosis requires exclusion of overlapping conditions:
| Condition | Key Distinguishing Feature |
|---|---|
| Generalized Anxiety Disorder (GAD) | Worries concern real-life problems; no compulsions |
| Major Depressive Disorder | Rumination is mood-congruent and ego-syntonic |
| Specific Phobia | Fear is circumscribed; no compulsions |
| Schizophrenia | Thought disorder, negative symptoms; intrusions are typically ego-syntonic |
| Body Dysmorphic Disorder | Obsessions exclusively about physical appearance |
| Hoarding Disorder | Distress related to discarding, without other OCD features |
| Tic Disorders / Tourette Syndrome | Premonitory urge without cognitive obsessional content |
| OCPD (Obsessive-Compulsive Personality Disorder) | Pervasive pattern of perfectionism; ego-syntonic; no discrete obsessions or compulsions |
Laboratory and Neuroimaging Investigations of OCD
There are no diagnostic biomarkers or laboratory tests specific to OCD. Investigations are indicated to exclude organic causes or comorbidities:
- Routine bloods: Full blood count, metabolic panel, thyroid function tests (hyperthyroidism can mimic anxiety), and drug screen
- Anti-streptococcal antibodies (ASO/anti-DNase B): In cases of suspected PANDAS, particularly with acute-onset OCD in children
- Neuroimaging (MRI/fMRI): Not routinely indicated, but may be used in atypical presentations or when organic pathology is suspected. Research applications demonstrate consistent OFC and caudate hyperactivity.
- EEG: Indicated when seizure activity or paroxysmal neurological symptoms coexist
- Genetic testing: Not currently part of standard clinical workup; may become relevant as pharmacogenomics advances
Complications of OCD
OCD is associated with significant multisystem morbidity when inadequately treated or unrecognized.
1. Psychiatric Complications
Major depressive disorder is the most common comorbidity, occurring in approximately 67% of individuals with OCD over their lifetime. Comorbid depression is associated with increased symptom severity, reduced treatment response, and elevated suicide risk — lifetime suicidal ideation is reported in up to 50% of OCD patients, and suicidal behavior in approximately 25%. Other frequent comorbidities include other anxiety disorders, eating disorders, and substance use disorders.
2. Neurological and Cognitive Complications
Chronic, unremitting OCD is associated with progressive cognitive impairment in domains of executive function, verbal fluency, and working memory. In pediatric-onset OCD, there is potential impact on neurodevelopment and academic attainment.
3. Cardiovascular Complications
Chronic psychological stress activates the hypothalamic-pituitary-adrenal (HPA) axis and sympathetic nervous system, contributing to sustained elevations in cortisol and catecholamines. This dysregulation is associated with hypertension, increased cardiovascular risk, and — in severe cases — cardiac arrhythmias.
4. Gastrointestinal Complications
Stress-mediated gut-brain axis dysregulation increases susceptibility to irritable bowel syndrome (IBS) and gastroesophageal reflux disease (GERD). These conditions may further exacerbate anxiety, creating a bidirectional feedback cycle.
5. Psychosocial and Functional Complications
OCD frequently leads to severe occupational and academic impairment, social isolation, and relationship dysfunction. Family members are significantly affected, often engaging in accommodation behaviors that inadvertently reinforce the disorder. The economic burden includes both direct treatment costs and substantial indirect costs from lost productivity.
Treatment of OCD
Treatment of OCD is most effective when individualized, combining evidence-based psychotherapy with pharmacotherapy as indicated. The overarching goal is symptom reduction sufficient to restore functional capacity, rather than symptom elimination (which may be an unrealistic target in severe OCD).
1. First-Line Psychotherapy: Exposure and Response Prevention (ERP)
ERP, a structured form of Cognitive-Behavioral Therapy (CBT), is the most empirically validated psychological treatment for OCD and is recommended as first-line therapy in all evidence-based guidelines (APA, NICE, CANMAT). ERP involves two components:
- Exposure: Systematic, graduated confrontation with feared stimuli (situations, objects, thoughts) without avoidance
- Response Prevention: Resisting the urge to engage in compulsive behaviors or mental rituals following exposure
ERP works by promoting inhibitory learning — new associations between feared stimuli and non-catastrophic outcomes — thereby reducing the anxiety driving compulsive behavior. Typical treatment involves 12–20 weekly sessions, with intensive formats (daily sessions) for severe cases. Response rates of 60–83% have been reported in controlled trials.
Cognitive interventions are often integrated with ERP to target dysfunctional beliefs, including cognitive restructuring addressing inflated responsibility, overestimation of threat, and thought-action fusion.
2. First-Line Pharmacotherapy: SSRIs
Selective serotonin reuptake inhibitors (SSRIs) are the first-line pharmacological treatment for OCD. Approved agents include:
| Agent | Typical OCD Dose Range | Notes |
|---|---|---|
| Fluoxetine | 40–80 mg/day | FDA-approved; long half-life useful in adherence difficulties |
| Fluvoxamine | 100–300 mg/day | FDA-approved; significant CYP450 interactions |
| Sertraline | 100–200 mg/day | FDA-approved; well-tolerated |
| Paroxetine | 40–60 mg/day | FDA-approved; discontinuation syndrome risk |
| Escitalopram | 20–40 mg/day | Not FDA-approved for OCD but widely used |
Key prescribing principles:
- OCD typically requires higher SSRI doses than those used for depression
- Full therapeutic response may take 8–12 weeks; an adequate trial is a minimum of 10–12 weeks at the maximum tolerated dose
- Partial responders should not be switched prematurely; augmentation is preferred
3. Second-Line Pharmacotherapy: Clomipramine
Clomipramine, a tricyclic antidepressant with potent serotonin reuptake inhibition, was the first medication approved for OCD. It is as efficacious as SSRIs but its use is limited by a less favorable side-effect profile (anticholinergic effects, cardiac QTc prolongation, seizure risk at high doses) and requires baseline ECG. It is typically reserved for SSRI non-responders or as augmentation.
4. Augmentation Strategies (Treatment-Resistant OCD)
Approximately 40–60% of patients show only partial response to initial SSRI treatment. Evidence-based augmentation strategies include:
- Low-dose atypical antipsychotics: Risperidone (0.5–2 mg/day) and aripiprazole have the strongest evidence base. Addition to SSRIs is beneficial in approximately 30–50% of partial responders.
- Clomipramine + SSRI combination: Used cautiously due to pharmacokinetic interactions (SSRIs raise clomipramine levels); requires ECG monitoring.
- Intensifying ERP: Adding or intensifying psychotherapy in pharmacological partial responders is strongly recommended before escalating to neuromodulation.
5. Neuromodulation and Investigational Therapies
For severe, treatment-resistant OCD (typically defined as failure of ≥2 adequate SSRI trials plus adequate ERP):
- Deep Brain Stimulation (DBS): FDA humanitarian device exemption granted for treatment-refractory OCD. Electrodes are implanted in targets such as the anterior limb of the internal capsule (ALIC) or the subthalamic nucleus. Approximately 50–60% of carefully selected patients achieve meaningful symptom reduction.
- Transcranial Magnetic Stimulation (TMS): Non-invasive repetitive TMS (rTMS) targeting the supplementary motor area (SMA) or OFC has received FDA clearance as adjunctive treatment for OCD. It is well-tolerated and may offer benefit in patients unwilling or unable to undergo DBS.
- Ketamine: Early evidence suggests rapid-onset, transient anti-obsessional effects via NMDA receptor antagonism; currently investigational.
- Neuro-immunological approaches: Under investigation in PANDAS/PANS subtypes.
6. Special Populations
Pediatric OCD: ERP is first-line treatment. Fluoxetine, sertraline, and fluvoxamine are FDA-approved for pediatric OCD. A combination of ERP and SSRI is superior to either alone in moderate-to-severe cases. Family-based ERP addressing parental accommodation is essential.
OCD in Pregnancy: ERP is preferred as first-line. SSRIs are considered relatively safe but risk-benefit analysis is required; sertraline and fluoxetine have the most safety data. Neonatal adaptation syndrome is a recognized risk with late-pregnancy exposure.
OCD with Poor Insight: Standard ERP and SSRI treatment remains appropriate; motivational enhancement techniques may improve engagement. Antipsychotic augmentation may be considered earlier.
Prevention and Control of OCD
There is currently no established primary prevention strategy that definitively prevents OCD onset. However, a comprehensive public health approach can reduce risk, facilitate early recognition, and improve outcomes.
1. Reducing Environmental Risk
Early trauma-informed care programs and evidence-based parenting interventions can reduce adverse childhood experiences known to elevate OCD risk. Promoting secure attachment and healthy emotional regulation in children builds psychological resilience.
2. Early Identification and Intervention
Training primary care providers, pediatricians, school counselors, and mental health professionals in OCD recognition is essential. Given the characteristic delay in diagnosis, systematic screening in high-risk populations (e.g., children with tic disorders, individuals with a family history of OCD) is warranted. Brief validated screening tools such as the OCI-R can be incorporated into primary care workflows.
3. Cognitive and Psychological Resilience
Stress management programs, mindfulness-based interventions, and CBT-based preventive approaches that address intolerance of uncertainty and maladaptive cognitive styles may reduce symptom severity or delay onset in at-risk individuals. There is emerging evidence for transdiagnostic CBT programs targeting shared vulnerability factors across anxiety and OCD-spectrum disorders.
4. Family and Community Education
Psychoeducation for families reduces accommodation behaviors that perpetuate OCD symptoms. Community awareness campaigns reduce stigma, increase help-seeking, and challenge misconceptions (e.g., conflating OCD with ordinary preferences for tidiness). Destigmatization is particularly critical as shame and concealment are major barriers to treatment access.
5. Public Health Surveillance
Population-level monitoring of OCD prevalence, treatment uptake, and outcomes supports identification of underserved populations and informs resource allocation. Integration of OCD metrics into national mental health surveillance frameworks would improve the evidence base for public health interventions.
Prognosis of OCD
The natural course of OCD is typically chronic with fluctuating severity. Without treatment, spontaneous remission is uncommon (occurring in approximately 20% of cases). With appropriate treatment:
- Approximately 70% of patients achieve meaningful symptom reduction with combined ERP and SSRI therapy
- Full remission is achieved in approximately 12–25% of cases
- Partial response is the most common outcome; ongoing maintenance treatment is usually required
- Earlier age of treatment initiation, greater treatment adherence, milder baseline severity, and absence of comorbid personality disorders are associated with better prognosis
Prognostically adverse factors include poor insight, early onset, severe hoarding symptoms, comorbid tic disorder, and prominent family accommodation behaviors.
Frequently Asked Questions (Clinical FAQs)
1. How is OCD distinguished from normal intrusive thoughts?
Intrusive thoughts occur in up to 90% of the general population. What distinguishes OCD is not the content of the intrusion, but the individual's appraisal of it (as meaningful, dangerous, or morally significant), the resulting distress, and the behavioral response (compulsions, avoidance). OCD is diagnosed when these processes cause significant distress or functional impairment.
2. Is OCD a "cleanliness disorder"?
This is a common misconception. Contamination fears and washing compulsions represent only one symptom dimension. Many patients present with intrusive aggressive, sexual, or religious thoughts; symmetry obsessions; or fear of causing harm — symptoms that may not be recognized as OCD by patients or clinicians unfamiliar with its full clinical range.
3. When should OCD be referred to a psychiatrist?
Referral is indicated when: (a) diagnosis is uncertain; (b) symptoms are moderate to severe (Y-BOCS ≥16); (c) there is significant comorbidity, including depression with suicidal ideation; (d) the patient has failed an adequate SSRI trial; or (e) specialist psychotherapy is required.
4. How long should a pharmacological trial last before declaring it inadequate?
An adequate SSRI trial for OCD requires at least 10–12 weeks at the maximum tolerated dose (ideally at or near the top of the recommended OCD dose range). This is longer than the 4–6 week trials typical in depression. Premature switching before an adequate trial is a common cause of apparent treatment failure.
5. Does OCD increase suicide risk?
Yes. OCD is associated with significantly elevated lifetime rates of suicidal ideation (up to 50%) and suicidal behavior (up to 25%). Suicide risk assessment should be a routine component of OCD clinical management, particularly when comorbid depression, substance use, or significant functional impairment is present.
6. Can OCD be effectively treated with online or digital interventions?
Yes. Internet-delivered CBT with therapist support (iCBT/iERP) has demonstrated efficacy comparable to in-person therapy in randomized controlled trials. Digital therapeutics represent a significant opportunity to address treatment gaps caused by limited access to specialist providers.
7. What is the role of support groups?
Peer support groups — whether in-person or online — can be valuable adjuncts to formal treatment. They reduce isolation, normalize experiences, and provide practical coping strategies. Clinicians should be aware, however, that unguided support groups carry a risk of inadvertent reassurance-giving, which may reinforce compulsions; this should be discussed with patients.
8. Can children develop OCD, and how does it differ from adult presentation?
Yes. Pediatric OCD often presents with prominent contamination, symmetry, and harm obsessions. Compulsions may be more behavioral and less internalized than in adults. Children may have limited insight and are more likely to involve family members in rituals (accommodation). A family-based ERP approach is essential in pediatric cases.
References
The following reference list should be populated with primary literature and evidence-based guidelines. Key sources to include:
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th Edition (DSM-5-TR). Washington, DC: APA; 2022.
- Abramowitz JS, Taylor S, McKay D. Obsessive-compulsive disorder. Lancet. 2009;374(9688):491–499.
- Fineberg NA, et al. The size, burden and cost of disorders of the brain in the UK. J Psychopharmacol. 2013;27(9):761–770.
- Goodman WK, et al. The Yale-Brown Obsessive Compulsive Scale (Y-BOCS). Arch Gen Psychiatry. 1989;46(11):1006–1016.
- Fontenelle LF, et al. The analytical epidemiology of obsessive-compulsive disorder: risk factors and correlates. Prog Neuropsychopharmacol Biol Psychiatry. 2011;35(1):1–8.
- Pittenger C, Bloch MH. Pharmacological treatment of obsessive-compulsive disorder. Psychiatr Clin North Am. 2014;37(3):375–391.
- Rosa-Alcázar AI, et al. Psychological treatment of obsessive-compulsive disorder: a meta-analysis. Clin Psychol Rev. 2008;28(8):1310–1325.
- Simpson HB, et al. Cognitive-behavioral therapy vs risperidone for augmenting serotonin reuptake inhibitors in obsessive-compulsive disorder. JAMA Psychiatry. 2013;70(11):1190–1199.
- Pallanti S, Hollander E, Bienstock C, et al. Treatment non-response in OCD: methodological issues and operational definitions. Int J Neuropsychopharmacol. 2002;5(2):181–191.
- NICE Clinical Guideline CG31. Obsessive-Compulsive Disorder and Body Dysmorphic Disorder: Treatment. National Institute for Health and Care Excellence; 2005 (updated 2019).