











Erythrocyte Sedimentation Rate (ESR) : Significance, Mechanism, Influencing factors, Biological Reference & Procedure
The Erythrocyte Sedimentation Rate (ESR) test is a commonly performed in the Hematology laboratory for the prognostic purpose that may indicate and monitor an increase in inflammatory activity within the body caused by one or more conditions such as chronic inflammatory disease, autoimmune disease, anemia, infections, and malignancies. The ESR test is not specific for any single disease but is used in combination with other tests to determine the presence of increased inflammatory activity. The ESR has long been used as a "sickness indicator" due to its reproducibility in both hematological and non hematological. When anticoagulated blood is allowed to stand undisturbed condition for a period of time, the erythrocytes tends to sink to the bottom. Two layers are formed, the upper plasma layer and lower sedimented erythrocyte layer. The rate at which the red cells fall is knows as Erythrocyte Sedimentation Rate (ESR).
Mechanism of sedimentation of RBCs :
The ESR is consist of mainly four phases. These are aggregation, rouleaux formation, sedimentation and packing.
- 1st 15 minutes : Phase of minimum fall : The red cells suspended in a column of citrated blood undergo rouleaux formation in the plasma and become heavier. Sedimentation in this phase is very low.
- 2nd 15 minutes : Phase of moderate falling : Fibrinogen and globulin in the plasma develop fine threads and build up a network. The rouleaux of the red cells get tapped in the mash of network and become heaviest. It starts to settle quickly.
- 3rd 15 minutes : Phase of maximum fall : In this phase the rate of fall of the protein network with red cell mass is maximums.
- 4th 15 minutes : Phase of packing : In this phase the sedimented red blood cells and protein mass undergoes packing to the bottom.
Factors influencing ESR :
- Plasma : RBCs carry a negative electronic charge, where as plasma carries a positive charge. Any conditions in plasma that increases it positive charge; increase rouleaux formation and increases ESR by lengthing stage-I (aggregation and rouleaux formation.). Fibrinogen, globulin and cholesterol accelerate while albumin retards sedimentation. Hence, ESR is increase in any conditions that increases fibrinogen (tissue break-down as in infection and tuberculosis) or globulin (rheumatic fever, multiple myaloma and kala-azar).
- Red Blood Cells : Increase in blood cell counts as in Polycythemia retards sedimentation due to the jostling (or pushing one another) effect on the cells. Low blood cell count in anaemia tends to increase ESR. However, altered shaped of the RBCs as in Sickle cell anaemia and microcytic hypochromic anaemia tends to prevent rouleaux formation and decrease ESR. In Sickle cell anaemia the red cell resist to rouleaux formation that’s why ESR is decreased
- Physiological Variation : ESR is low in infants, increase upto puberty, and then decreases upto old age when aging it increased. ESR is greater in women then men. It increases after the third month of pregnancy and returns to normal by about third or fourth weeks after delivery (postpartum).
- Temperature of the environment : ESR is increases when temperature of the environment is increase. It is directly proportional to the temperature.
- Difference between specific gravity of Red blood cell and plasma.
- Diameter and length of the ESR tube.
- Position of the ESR tube : Normally ESR tube is placed vertical position (90°). If the tube is placed slightly slant, ESR is increases. For every 3° of the tube position ESR is increase approximately 30 mm.
Clinical Significance of ESR
The Erythrocyte Sedimentation Rate (ESR) is a nonspecific hematological test that reflects the presence and intensity of inflammation in the body. It measures the rate at which red blood cells settle in anticoagulated blood within one hour. Although ESR is not diagnostic for any specific disease, it has important prognostic and monitoring value in various clinical conditions. ESR has considerable prognostic significance. Variations in ESR levels help assess the course and progression of a disease. In conditions such as tuberculosis, rheumatic fever, multiple myeloma, and kala-azar, a markedly elevated ESR indicates active disease. When the ESR value gradually returns to normal, it generally suggests improvement or recovery. However, because ESR is a nonspecific indicator, it should always be interpreted in conjunction with clinical findings and other diagnostic tests.
Being a nonspecific test, ESR has certain limitations in clinical practice. It can be affected by numerous physiological and pathological factors, and therefore, it cannot be used to make a specific diagnosis. Despite these limitations, ESR remains a useful supportive investigation in appropriate clinical settings, particularly for screening, diagnosis, and monitoring disease activity or therapeutic response.
- Screening Applications
- Asymptomatic Patients
In the past, ESR was occasionally used as a general screening test. However, studies have demonstrated no significant value of ESR in screening asymptomatic individuals. Abnormal ESR results in healthy individuals are rare and usually return to normal within a few months without the emergence of any disease. Therefore, a detailed history and physical examination serve as a far better screening approach than ESR alone.
- Patients with Nonspecific Symptoms
When patients present with nonspecific complaints such as fatigue, malaise, or vague pain, a moderate elevation of ESR may justify further diagnostic evaluation. Such elevations are commonly seen in infectious diseases, inflammatory disorders, and malignancies. However, a normal ESR value does not exclude the possibility of underlying active disease.
- Diagnostic Applications
ESR is helpful as a supportive diagnostic tool in several inflammatory and vascular diseases.
- Temporal Arteritis and Giant Cell Arteritis : Temporal arteritis, a form of giant cell arteritis, involves inflammation of the temporal arteries and is considered a medical emergency. If not treated promptly, it may cause ophthalmic arterial thrombosis, resulting in permanent blindness. Definitive diagnosis requires histopathological examination of a temporal artery biopsy; however, biopsy results are often delayed. In such cases, an ESR value greater than 90 mm/hour (Wintrobe method) strongly supports the diagnosis, as 99% of patients show an ESR above 30 mm/1st hour. When symptoms are suggestive, an elevated ESR is an indication to initiate corticosteroid therapy immediately, even before biopsy confirmation. Giant cell arteritis may also involve other large arteries with vague systemic symptoms, where a very high ESR serves as a crucial diagnostic clue.
- Polymyalgia Rheumatica : Polymyalgia rheumatica (PMR) and giant cell arteritis are often considered part of the same disease spectrum. PMR presents with stiffness and pain in the shoulders, hips, and lower back, along with malaise, anemia, and an elevated ESR. Diagnosis is clinical and made after excluding other rheumatic, vasculitic, malignant, or chronic infectious disorders.
- Other Inflammatory Conditions : ESR is also used in the emergency department for the evaluation of conditions such as appendicitis, pelvic inflammatory disease, septic arthritis, and various other inflammatory diseases.
- Monitoring Disease Activity
ESR is widely used as a monitoring parameter to evaluate disease activity and response to treatment in inflammatory and autoimmune conditions.
- Temporal Arteritis and Polymyalgia Rheumatica : In these disorders, ESR values are usually markedly elevated. A gradual decline in ESR, accompanied by clinical improvement, indicates an effective therapeutic response. Conversely, persistent elevation of ESR, despite symptomatic relief, may signify poor or incomplete response to therapy.
- Rheumatoid Arthritis : In rheumatoid arthritis, about 90–95% of patients show elevated ESR levels. The ESR closely correlates with disease activity and mirrors clinical symptoms. A persistently high ESR is usually associated with active disease or poor prognosis.
- Collagen Vascular Diseases : Similar to rheumatoid arthritis, ESR generally parallels disease activity in other collagen vascular disorders, including systemic lupus erythematosus and systemic sclerosis.
- Neoplastic Conditions : A persistently high ESR is often associated with malignant diseases and correlates with poor prognosis. Cancers commonly showing elevated ESR include:
-
- Hodgkin’s disease
- Gastric carcinoma
- Renal cell carcinoma
- Chronic lymphocytic leukemia
- Breast, colorectal, and prostate cancers
In cases of solid tumors, an ESR exceeding 100 mm/hour usually indicates metastatic spread. However, due to its nonspecific nature, ESR has largely been replaced by modern diagnostic methods such as tumor markers and imaging studies.
Conditions Associated with Decreased ESR
ESR may be decreased in conditions that reduce plasma proteins or alter the shape and charge of red blood cells. These include:
-
- Hyperalbuminemia
- Congestive cardiac failure
- Hyperglycemia
- Hypofibrinogenemia
- Hypogammaglobulinemia
- Increased bile salts or phospholipids
- Hemoglobinopathies such as Hemoglobin C disease and sickle cell anemia
- Thalassemia, microcytosis, polycythemia, spherocytosis, acanthocytosis
- Severe dehydration (e.g., cholera, gastroenteritis)
- Hypochromic microcytic anemia
- Neonatal period, infancy, and old age
- Cachexia and chronic malnutrition
Conditions Associated with Increased ESR
ESR increases in all conditions involving tissue destruction, inflammation, necrosis, or the presence of foreign proteins in the bloodstream.
Common causes of elevated ESR include:
-
- Tuberculosis
- Rheumatic fever
- Myocardial infarction
- Kala-azar
- Rheumatoid arthritis
- Systemic lupus erythematosus
- Chronic osteomyelitis
- Chronic lung abscess
- Carcinomatosis (malignancy), leukemia, anemia, macrocytosis
- Hypercholesterolemia, hyperfibrinogenemia, hypergammaglobulinemia
- Hypoalbuminemia
- Acute heavy metal poisoning
- Acute bacterial infections
- Collagen vascular diseases
- Diabetes mellitus
- End-stage renal failure
- Gout
- Menstruation and pregnancy
- Syphilis
- Temporal arteritis
- Drug effects
Special Note:
In Multiple Myeloma, the ESR is markedly elevated, often ranging from 130–140 mm/hour in the first hour, due to excessive abnormal immunoglobulin production. Although ESR is a nonspecific test, it remains a valuable, cost-effective, and widely available indicator for the presence of inflammation and disease progression. Its greatest utility lies in monitoring the course of diseases such as rheumatoid arthritis, temporal arteritis, and polymyalgia rheumatica. However, interpretation should always be made in conjunction with clinical evaluation and other laboratory investigations to ensure diagnostic accuracy.
Determination of Erythrocyte Sedimentation Rate (ESR)
Determination of ESR is done by several methods. These are as follows:
In the developing countries former two methods are used for ESR determination in the laboratory.
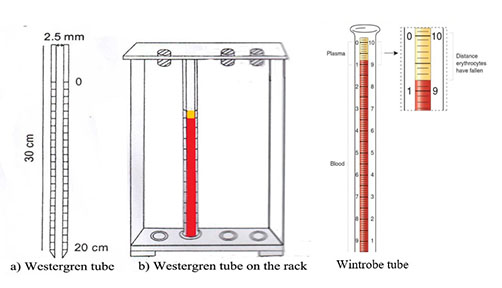
Wintrobe’s tube :
- It is 110 mm long tube with a 3.0 mm internal bore. It is graduated from ‘0’ upto ‘100’ mm (10 cm). The scale with the descending order is used for ESR determination.
- It is also used for Packed Cell determination.
Westergren’s tube :
- It is 300 mm long tube with a 2.5 mm internal bore. It is graduated from ‘0’ upto ‘200’ mm (20 cm). The scale with descending order is used for ESR determination.
- It is more specific then the Wintrobe’s method and others methods.
Normal value :
- By Westergren’s method :
- Male : 0-15 mm/1st hour
- Female : 0-20 mm/ 1st hour
- By Wintrobe’s method :
- Male : 0-9 mm/1st hour
- Female : 0-20 mm/ 1st hour
Biological Reference Interval :
|
Gender |
Age | Biological Reference | Unit |
|
|
0 – 28 Days | 0 - 2 |
mm/1st hr. |
|
|
28 Days – 16 Yrs. | 3 - 13 |
mm/1st hr. |
|
Male |
61 – 70 Yrs. | ≤ 14 |
mm/1st hr. |
|
Male |
> 70 Yrs. |
≤ 30 |
mm/1st hr. |
|
Female |
17-50 Yrs. |
≤ 12 |
mm/1st hr. |
|
Female |
51-60 Yrs. |
≤ 19 |
mm/1st hr. |
|
Female |
61-70 Yrs. |
≤ 20 |
mm/1st hr. |
| Female | > 70 Yrs. |
≤ 35 |
mm/1st hr. |
DETERMINATION OF ERYTHROCYTE SEDIMENTATION RATE BY WESTERGREN'S METHOD
Principle of the Test :
When anticoagulated blood is allowed to stand undisturbed condition for a period of time, the erythrocytes tends to sink to the bottom. Two layers are formed, the upper plasma layer and lower sedimented erythrocyte layer. The rate at which the red cells fall is knows as Erythrocyte Sedimentation Rate (ESR) and give the result as mm/1st hour.
Specimen :
Patient should be fasting for 12 to 16 hours. Collect venous blood. 2.0 ml of blood is collected in a vial containing 0.5 ml of 3.8% Sodium citrate anticoagulant. Fasting EDTA (Ethyl Di-amine Tetra Acetic acid) anticoagulated whole blood is also used for ESR determination.
Requirements :
- Westergren’s tube with stand.
- Test tube with test tube rack.
- 3.8 % Sodium Citrate solution.
- Stop watch.
- Blood drawer.

Procedure :
- Blood drawer attached with clean and dry Westergren’s tube.
- Drawn 3.8% sodium citrate upto ‘150’ mark from ‘200’ mark in a test tube.
- Drawn well mixed anticoagulated blood upto ‘0’ mark from ‘200’ mark of the tube and mixed with 3.8% sodium citrate present in the test tube.
- Mixed well, filled the Westergren tube exactly upto ‘0’ mark (avoid air babbles formation in the tube).
- Placed the tube upright position in the ESR stand, it should fit evenly into the groove of the stand and it allowed standing undisturbed condition exactly for 1 hour. Set the time in Stop-watch.
- Exactly after 1 hour, note the level to which the red cell column has fallen.
- Report the result in terms of mm/1st hour.
DETERMINATION OF ERYTHROCYTE SEDIMENTATION RATE BY WINTROBE'S METHOD
Principle of the Test :
When anticoagulated blood is allowed to stand undisturbed condition for a period of time, the erythrocytes tends to sink to the bottom. Two layers are formed, the upper plasma layer and lower sedimented erythrocyte layer. The rate at which the red cells fall is knows as Erythrocyte Sedimentation Rate (ESR) and give the result as mm/1st hour.
Specimen :
Fresh fasting (12 to 16 hours fasting) Ethyl Di-amine Tetra Acetic acid (EDTA) anticoagulated and undiluted whole blood.
Requirement :
- Wintrobe’s tube with stand.
- Special Pasteur pipette attached with rubber tied.
- Stop watch.
Procedure :
- Mixed the blood carefully in the vial.
- Filled the Wintrobe's tube to the ‘0’ mark by using a special Pasteur pipette.
- Placed the tube in exact vertical position in the stand.
- Set the Stop-watch for 1 hour.
- At the end of one hour note the level of erythrocyte column and give the result in terms of mm after first one hour (mm/ 1st hour).
References :
- Practical Hematology, Dacie & Lewis: 12th edition
- Clinical Diagnosis & management by laboratory methods, Henry’s: 21st edition
- Text Book of Medical Laboratory Technology, Dr. P.B. Godkar & Dr. D.P. Godkar : 5th edition
- Practical Medicine, P.J. Mehta’s : 20th edition