










Dengue Fever – Sign and Symptoms, Risk Factors, Diagnosis, Complications, Treatment and Prevention
Dengue fever is the most rapidly spreading mosquito-borne arboviral disease in the world, caused by the dengue virus (DENV) — a single-stranded, positive-sense RNA virus belonging to the genus Flavivirus, family Flaviviridae. It exists as four antigenically distinct but related serotypes: DENV-1, DENV-2, DENV-3, and DENV-4. Globally, an estimated 390 million dengue infections occur annually, of which approximately 96 million manifest clinically, and 3.9 million represent severe dengue — making dengue a leading cause of febrile illness, hospitalization, and mortality in tropical and subtropical regions. The World Health Organization classifies dengue as one of the top ten threats to global health, and the disease is now endemic in over 128 countries, placing approximately 3.9 billion people at risk of infection. The first half of 2024 saw a record-breaking 5.2 million reported cases globally — a dramatic doubling attributed to El Niño-driven climate changes, accelerating urbanization, and expanding mosquito vector ranges. 
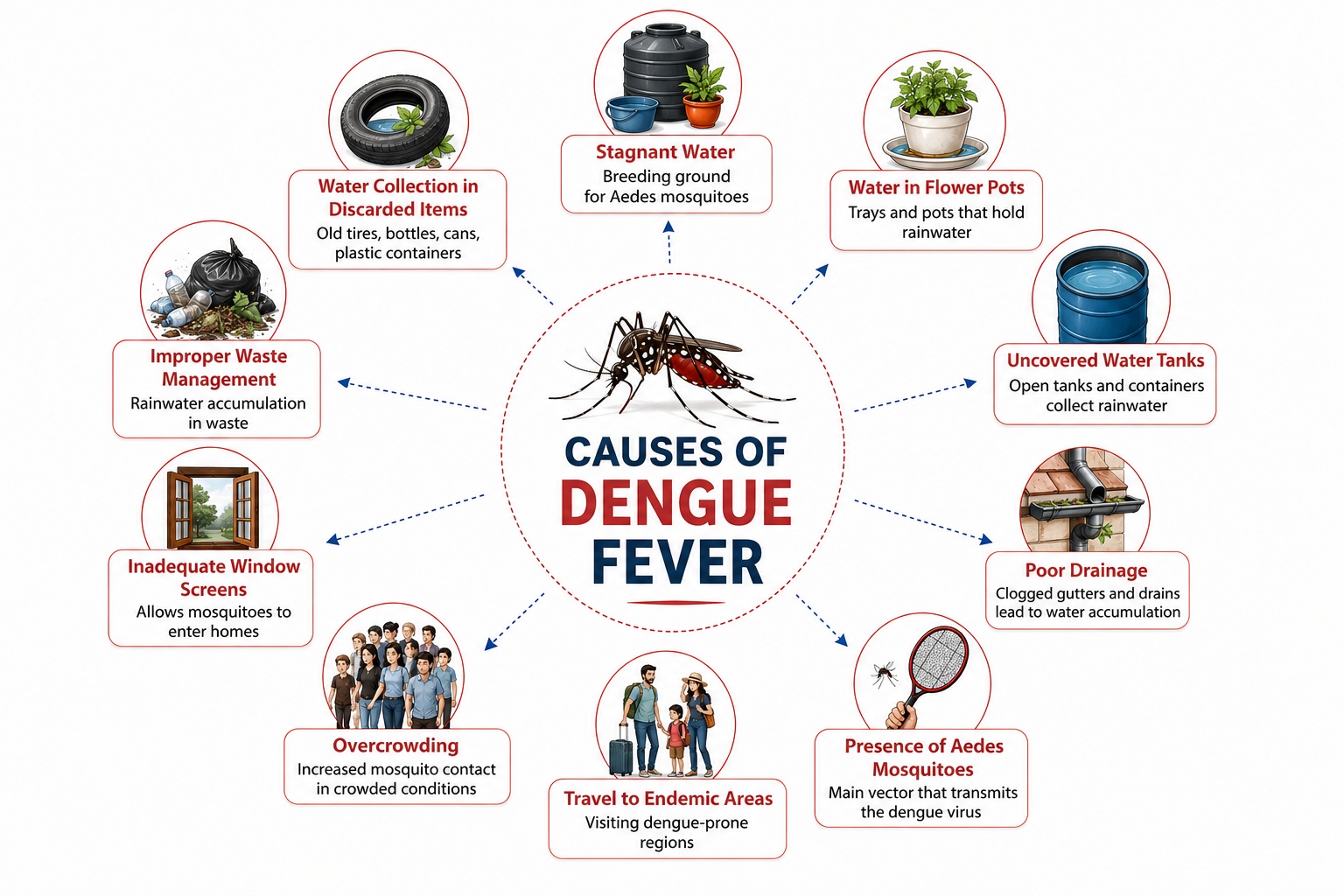
The primary vector, Aedes aegypti — a peridomestic, day-biting mosquito that thrives in urban environments and breeds in small collections of standing water (flower pots, discarded tyres, water storage containers, blocked drains) — is responsible for the majority of dengue transmission globally. The secondary vector, Aedes albopictus (tiger mosquito), has extended dengue transmission into previously non-endemic temperate regions of Europe, North America, and East Asia. The dengue virus is transmitted to humans through the bite of an infected female Aedes mosquito during its blood meal. Following an intrinsic incubation period of 4–10 days, the virus replicates in skin dendritic cells (Langerhans cells), disseminates via the lymphatics to regional lymph nodes, enters monocytes and macrophages (its primary target cells), undergoes systemic viremic dissemination, and triggers a complex inflammatory cascade through antibody-dependent enhancement (ADE), cytokine storm, complement activation, and endothelial dysfunction that underpins the full spectrum of dengue pathology.
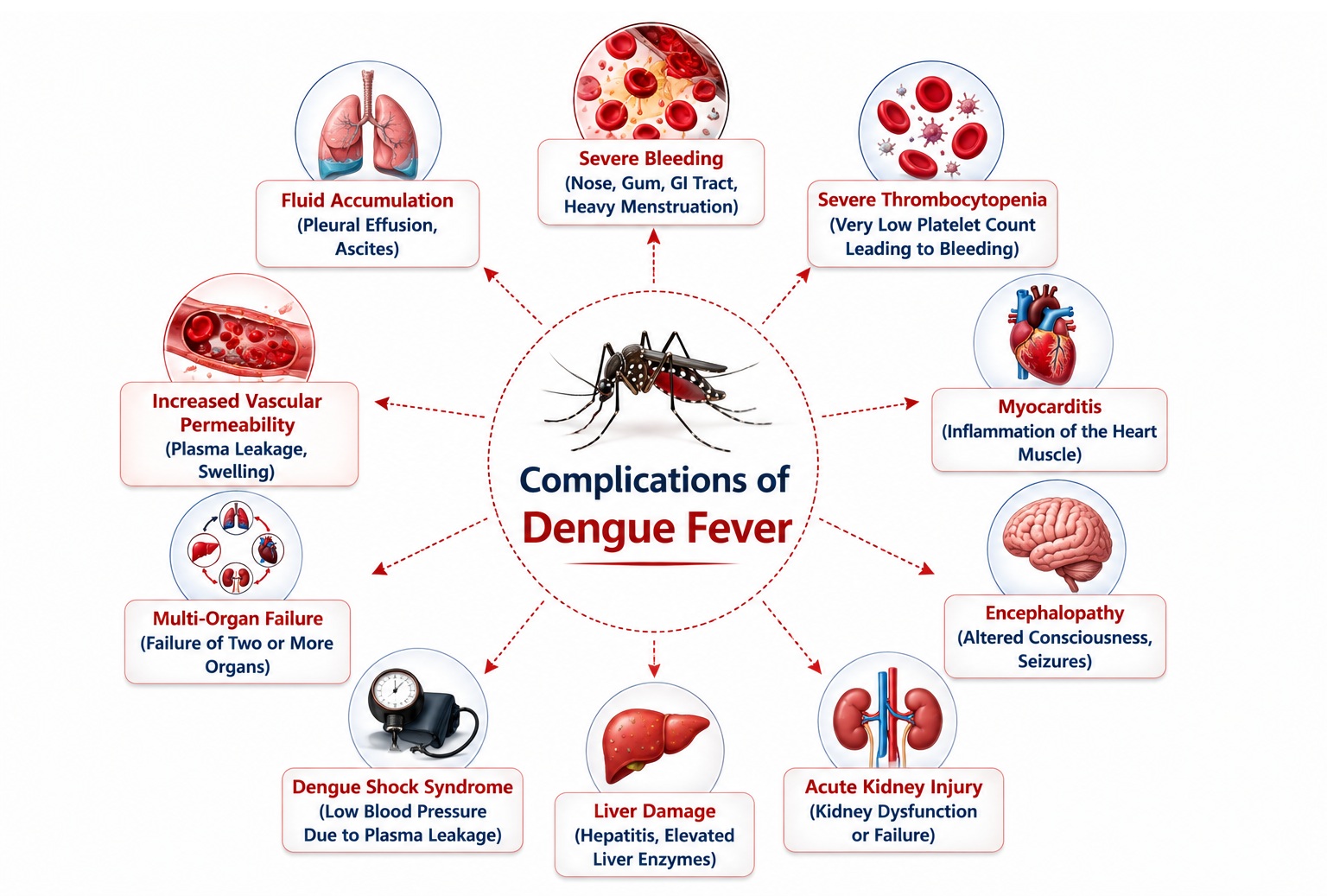
Dengue manifests as a clinical triad of sudden high fever, severe headache with retro-orbital pain, and severe myalgia/arthralgia — historically termed "break-bone fever" for its characteristic debilitating bone and joint pain. The 2009 WHO classification stratifies dengue into dengue without warning signs, dengue with warning signs (the critical category requiring close monitoring to prevent progression), and severe dengue (dengue hemorrhagic fever — DHF; dengue shock syndrome — DSS; severe organ impairment). The pathognomonic feature distinguishing simple dengue from DHF is plasma leakage — caused by increased vascular permeability from cytokine-driven endothelial dysfunction — resulting in hemoconcentration, pleural effusions, ascites, and potentially hypovolemic shock (DSS) when severe. Secondary dengue infection with a different serotype markedly amplifies disease severity through antibody-dependent enhancement (ADE) — pre-existing non-neutralizing cross-reactive antibodies from the primary infection opsonize the new serotype, facilitating enhanced monocyte-macrophage viral entry and dramatically amplifying cytokine production and inflammatory cascades.
Management remains supportive — there are no approved specific antiviral therapies for dengue. The cornerstone of dengue management is meticulous fluid balance, judicious intravenous fluid administration during the critical phase to compensate for plasma leakage while avoiding fluid overload, platelet monitoring and transfusion in severe thrombocytopenia with active bleeding, and vigilant clinical and laboratory monitoring for the transition from warning signs to severe dengue. Two vaccines are now approved: Dengvaxia (CYD-TDV, Sanofi Pasteur) for seropositive individuals aged 9–45 years in endemic countries, and Qdenga (TAK-003, Takeda) — a live-attenuated tetravalent dengue vaccine demonstrating efficacy even in seronegative recipients and now approved in multiple countries. Vector control — targeting Aedes breeding sites, larval control, and innovative biological control strategies including Wolbachia-infected mosquito releases — remains the primary prevention strategy at the population level.
Classification of Dengue Fever
The WHO 2009 Classification — which replaced the older 1997 WHO classification (dengue fever, DHF grades I–IV, DSS) — stratifies dengue by clinical severity and the presence of warning signs, directly guiding triage, monitoring intensity, and clinical decision-making:
| WHO 2009 Category | Clinical Features | Management Level |
|---|---|---|
| Dengue Without Warning Signs | Fever + ≥2 of: nausea/vomiting, rash, aches/pains, leukopenia, positive tourniquet test; confirmed or probable dengue | Home management; daily clinical review; oral hydration; return instructions for warning signs |
| Dengue With Warning Signs | Abdominal pain, persistent vomiting, clinical fluid accumulation, mucosal bleeding, lethargy, liver enlargement >2 cm, rapid rise in haematocrit with rapid platelet fall | Hospital admission; close observation; IV fluids if indicated; parenteral monitoring every 2–4h |
| Severe Dengue | Severe plasma leakage (shock, respiratory distress) OR severe bleeding OR severe organ impairment (liver: ALT/AST >1000 U/L; CNS: impaired consciousness; cardiac; kidneys) | Urgent high-dependency / ICU admission; IV fluid resuscitation; blood products; specialist care |
The Three Clinical Phases of Dengue
- Febrile Phase (Days 1–3) : Sudden high fever (39–40°C); flushed face; skin erythema; myalgia; arthralgia; headache; retro-orbital pain; anorexia; nausea. Mild haemorrhagic manifestations (petechiae, positive tourniquet test). WBC begins to fall. Febrile seizures possible in children.
- Critical Phase (Days 4–6) : Defervescence (fever breaks). Plasma leakage peaks — pleural effusion, ascites, hemoconcentration (HCT rise ≥20%). Platelet nadir. Risk of DSS (cold extremities, narrow pulse pressure, hypotension). Organ impairment may develop. Warning signs must be actively sought.
- Recovery Phase (Days 7–10) : Plasma reabsorption; haematocrit normalises; platelet count recovers; bradycardia common (vagal); "recovery rash" — white islands on red background (isles of white in sea of red). Risk of fluid overload from reabsorption if IV fluids not stopped in time.
Dengue Hemorrhagic Fever (DHF) — Older Grading (WHO 1997)
The older WHO 1997 grading remains clinically referenced in many settings. DHF is defined by ALL four criteria: fever (2–7 days), haemorrhagic tendency (positive tourniquet test, petechiae, ecchymosis, or mucosal bleeding), thrombocytopenia (≤100,000/mm³), and plasma leakage (haematocrit rise ≥20% or fall ≥20% after fluid replacement; pleural effusion or ascites):
| DHF Grade | Features | Designation |
|---|---|---|
| Grade I | Fever + nonspecific constitutional symptoms + positive tourniquet test; thrombocytopenia + plasma leakage (haemoconcentration) | DHF without shock |
| Grade II | Grade I + spontaneous bleeding (skin, gums, GI tract, injection sites) | DHF without shock |
| Grade III | DHF + circulatory failure: rapid/weak pulse, narrow pulse pressure ≤20 mmHg, hypotension, cold clammy skin, restlessness | Dengue Shock Syndrome (DSS) |
| Grade IV | Profound shock: undetectable blood pressure and pulse | Dengue Shock Syndrome (DSS) — profound |
Signs and Symptoms of Dengue Fever
After an incubation period of 4–10 days (range 3–14 days) following an infective mosquito bite, dengue presents with a characteristic constellation of symptoms. The clinical manifestation ranges from completely asymptomatic infection (approximately 75% of DENV infections) to severe, life-threatening dengue — determined by host immune status, viral serotype and strain virulence, prior dengue exposure, and host genetic factors.
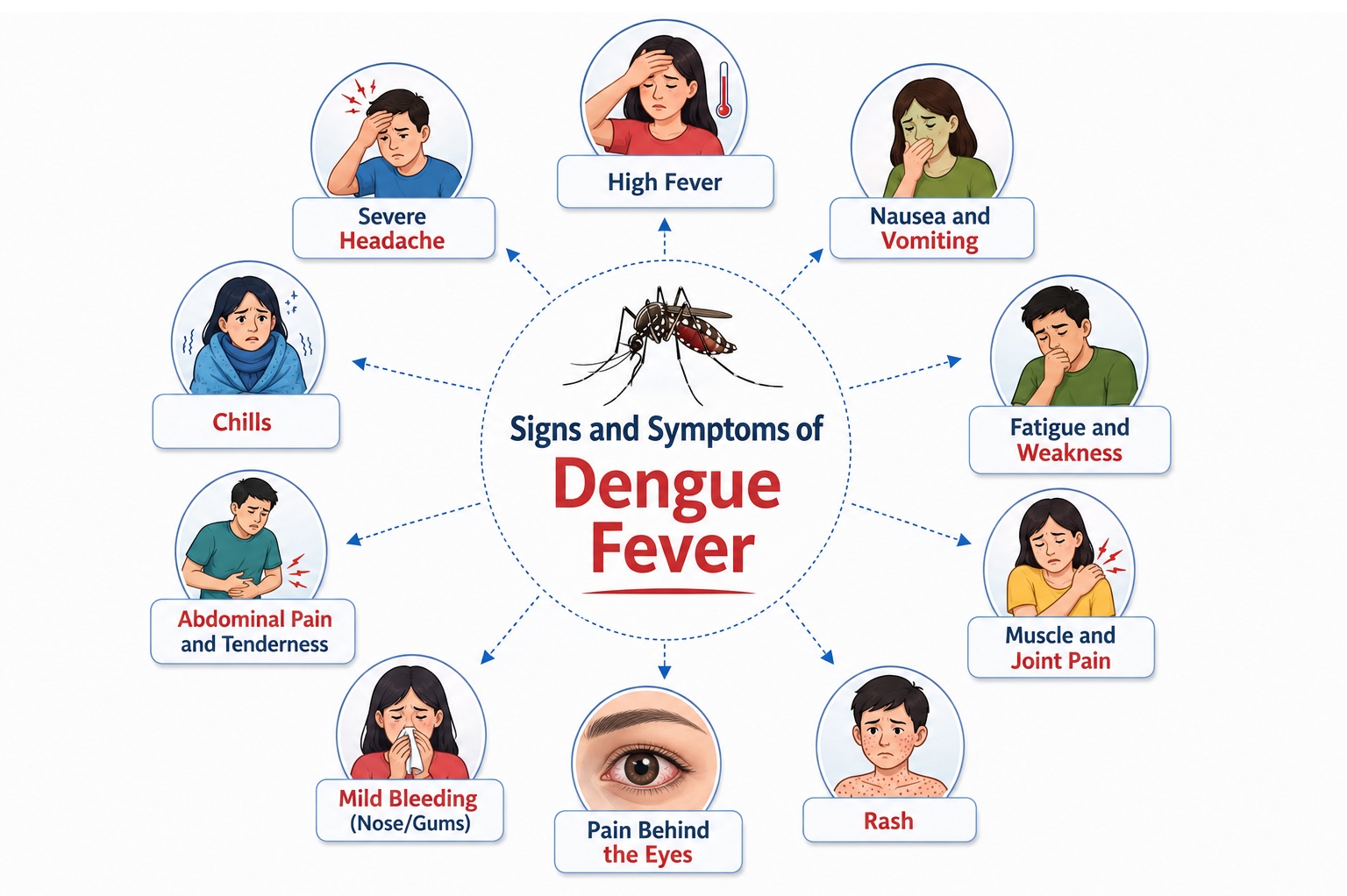
1. Fever and Constitutional Symptoms
- Sudden onset high fever (39–40°C): The most defining clinical feature — fever in dengue is typically abrupt in onset, reaching 39–40°C (occasionally 41°C) within hours, without a prodrome. The fever pattern is characteristically biphasic (saddle-back or camel-back pattern) in classical dengue: the initial febrile episode of 3–4 days is followed by a brief 24-hour afebrile period, then a second fever spike of 1–2 days — a pattern that, while not present in all cases, is clinically useful when observed. The fever is accompanied by profound systemic symptoms and does not respond adequately to antipyretics alone during the acute phase. Defervescence (fever breaking, typically around days 3–5) heralds the onset of the critical phase, when vascular permeability peaks and clinical deterioration can occur paradoxically despite apparent temperature improvement.
- Severe headache: An intense, persistent frontal or retro-orbital headache is among the most reported symptoms, present in >90% of symptomatic dengue patients. The pain behind the eyes is particularly characteristic — retro-orbital pain that is typically aggravated by eye movement and accompanied by photophobia. The headache reflects central nervous system effects of the viremia and inflammatory mediator burden, along with direct action of dengue viral proteins on pain-sensitive meningeal structures.
- Myalgia and arthralgia — "Breakbone Fever": Dengue acquired its historical sobriquet "breakbone fever" or "bonecrusher disease" from the extraordinarily severe, diffuse muscle pain (myalgia), joint pain (arthralgia), and bone pain that accompanies the acute febrile phase. Pain is particularly intense in the lumbar back muscles, thigh muscles, calf muscles, and periarticular regions of the knees, ankles, and wrists. The mechanism involves direct viral invasion of skeletal muscle, prostaglandin-mediated inflammatory pain signaling, and cytokine (TNF-α, IL-1β, IL-6)-mediated pain hypersensitivity. The severity of musculoskeletal pain in dengue is virtually unlike that of any other common febrile illness and represents a defining clinical distinguishing feature.
- Prostration and profound fatigue: Patients with dengue are characteristically incapacitated by their illness — unable to carry out any normal activities, spending most of the febrile period in bed. This degree of functional impairment, arising from the combined effects of fever, pain, cytokine-mediated sickness behavior, and reduced oral intake, is disproportionately severe compared to other common febrile illnesses of comparable duration and helps clinicians recognize dengue in endemic settings.
- Anorexia, nausea, and vomiting: Loss of appetite and nausea are present in the majority of dengue patients during the febrile phase, mediated by the inflammatory cytokine burden, gastroparesis from autonomic dysfunction, and direct effects of dengue viremia on the gastrointestinal mucosa. Persistent vomiting that prevents adequate oral rehydration — defined as more than three episodes in 24 hours — is a specific WHO warning sign indicating risk of progression to severe dengue and mandates clinical evaluation for hospital-based IV fluid therapy.
- Flushing and facial erythema: A diffuse, blotchy erythematous flushing of the face, neck, and upper chest is a distinctive early feature of dengue, seen in the first 24–48 hours of fever. This results from generalized vasodilation and increased cutaneous blood flow mediated by vasoactive inflammatory mediators. The flushed appearance may be mistaken for sunburn in fair-skinned individuals or misattributed to other viral exanthems.
2. Rash in Dengue
- First-phase rash — early generalized erythema (Day 1–3): A transient, generalized macular erythematous rash may appear in the first 1–2 days of fever — blotchy, non-specific, blanching, and easily overlooked on darker skin tones. It represents the early cutaneous manifestation of dengue viremia and vascular dilation. This rash typically fades within 24–48 hours and is clinically less diagnostically useful than the second-phase rash.
- Second-phase "dengue rash" — isles of white in a sea of red (Day 4–7): The characteristic and highly recognizable second rash of dengue appears during or just after defervescence (around days 4–6), corresponding to the critical-to-recovery transition phase. It presents as a maculopapular or morbilliform (measles-like) eruption with a striking and pathognomonic pattern: areas of normal-appearing (white) skin surrounded by a confluent erythematous (red) background — aptly described as "isles of white in a sea of red" or "white islands on a red sea." The rash typically begins on the torso and spreads centrifugally to the extremities, sparing the palms and soles in many cases. It is accompanied by pruritus (itching) in approximately 50% of patients and may desquamate (peel) as it resolves. The second dengue rash is highly characteristic and serves as an important clinical clue to dengue diagnosis during the critical-to-recovery transition.
- Petechiae: Tiny, non-blanching, pinpoint hemorrhagic spots (1–2 mm diameter) appearing in the skin — particularly on the lower limbs, trunk, and periorbital regions — represent capillary hemorrhage from thrombocytopenia and endothelial dysfunction. Petechiae may appear as early as day 3 of illness and become more prominent as the platelet count falls below 50,000/mm³. Distribution of petechiae may be accentuated in areas of venous stasis or external pressure (dependent areas, belt lines, elastic bands).
- Positive tourniquet test (Rumple-Leede test): A standardized clinical test for capillary fragility and a core dengue diagnostic criterion: a blood pressure cuff is inflated to a pressure halfway between systolic and diastolic for 5 minutes; the test is positive (and strongly suggestive of dengue) if 10 or more petechiae appear per square inch (2.5 × 2.5 cm) area in the antecubital fossa. A positive tourniquet test reflects the combination of thrombocytopenia and increased capillary fragility from endothelial dysfunction — it is positive in >80% of dengue patients by the end of the febrile phase and represents both a diagnostic criterion for dengue and an early warning of hemorrhagic tendency.
3. Hemorrhagic Manifestations
- Minor hemorrhagic manifestations (common in all dengue grades): Petechiae, epistaxis (nosebleeds), gingival bleeding (bleeding gums), easy bruising (ecchymosis), and menorrhagia (heavier-than-normal menstrual bleeding) represent the most frequent hemorrhagic features, arising from the combination of thrombocytopenia and platelet dysfunction. These manifestations, while concerning and requiring monitoring, do not in themselves indicate severe dengue unless accompanied by significant volume loss or plasma leakage.
- Major hemorrhagic manifestations (WHO Severe Dengue): Gastrointestinal hemorrhage (hematemesis — vomiting blood; melena — black tarry stools; frank rectal bleeding — hematochezia), gross hematuria (blood in urine), hemoptysis (blood in sputum), and intracranial hemorrhage represent serious, life-threatening hemorrhagic complications that require immediate hospital management, blood product support, and monitoring for hemodynamic instability. GI hemorrhage is the most clinically significant hemorrhagic complication, capable of causing fatal exsanguination in dengue shock syndrome.
- Vaginal bleeding: Women of reproductive age may experience unusually heavy menstrual bleeding or breakthrough bleeding during dengue illness, attributed to thrombocytopenia, platelet dysfunction, and hormonal effects of the febrile illness. Heavy vaginal bleeding in the context of severe thrombocytopenia (<20,000/mm³) may require platelet transfusion.
4. Warning Signs — Critical Clinical Recognition
(1) Abdominal pain or tenderness · (2) Persistent vomiting (>3 episodes in 24h) · (3) Clinical fluid accumulation (ascites, pleural effusion) · (4) Mucosal bleeding (not just petechiae) · (5) Lethargy or restlessness / irritability · (6) Liver enlargement >2 cm · (7) Laboratory: rapid rise in haematocrit concurrent with rapid fall in platelet count. These warning signs typically appear around the time of defervescence (Days 3–7) and mark the transition into the critical phase. Missing them delays life-saving fluid management.
- Abdominal pain and tenderness: A new onset of severe or persistent abdominal pain — particularly epigastric or right upper quadrant pain — is one of the most reliable warning signs of impending plasma leakage, hepatic involvement, or peritoneal accumulation of leaked plasma as ascites. Right upper quadrant tenderness reflects hepatic congestion and early hepatitis from dengue-associated liver injury. Acute abdomen mimicry from massive ascites or right-sided pleural effusion can challenge surgical differential diagnosis.
- Lethargy, restlessness, and altered mental status: A sudden change in the level of consciousness or behavior — from the child who was previously energetic suddenly becoming unresponsive, or from the patient who was resting becoming acutely restless and agitated — is a critical warning sign of early compensated or decompensated dengue shock. Restlessness and anxiety may signal impending circulatory collapse from plasma leakage, while lethargy or confusion suggests reduced cerebral perfusion. Any alteration in consciousness or behavior in a dengue patient mandates immediate clinical assessment of circulatory status.
- Liver enlargement (>2 cm below costal margin): Hepatomegaly, tender on palpation, detected on clinical examination is a WHO warning sign of dengue. Dengue virus infects hepatocytes, Kupffer cells, and sinusoidal endothelial cells, causing direct viral cytopathic injury and immune-mediated hepatocellular damage. Liver enlargement with right upper quadrant tenderness preceding or accompanying the critical phase warns of potentially severe hepatic involvement and risk of fulminant hepatitis.
- Rapid haematocrit rise with rapid platelet fall: The combination of rising haematocrit (hemoconcentration — haematocrit increase ≥20% over baseline or above age-sex-adjusted normal) with simultaneously falling platelet count is the laboratory signature of the dengue critical phase and plasma leakage. Serial haematocrit monitoring every 4–6 hours during the critical phase is the single most important laboratory parameter for dengue management decisions and guides IV fluid administration in DHF.
5. Manifestations of Severe Dengue (DHF / DSS)
- Dengue Shock Syndrome (DSS): The most life-threatening manifestation of dengue — representing the clinical consequences of severe plasma leakage causing hypovolemia and cardiovascular collapse. Clinical features evolve from compensated shock (tachycardia, narrow pulse pressure ≤20 mmHg despite normal or slightly reduced SBP, cold clammy peripheries, prolonged capillary refill time >3 seconds) to decompensated shock (overt hypotension: SBP <90 mmHg or mean arterial pressure <70 mmHg; undetectable pulse in grade IV DSS; diaphoresis; cyanosis; metabolic acidosis; altered consciousness). DSS typically occurs at defervescence (days 4–6) and can progress from early warning signs to irreversible shock within hours if not recognized and treated promptly with judicious IV fluid resuscitation.
- Dengue hepatitis and acute liver failure: Hepatic injury is common in dengue, ranging from asymptomatic transaminase elevation to acute liver failure. Alanine aminotransferase (ALT) and aspartate aminotransferase (AST) are elevated in virtually all dengue cases, typically peaking at the end of the febrile phase. ALT/AST >1000 IU/L constitutes a criterion for severe dengue. Dengue-associated acute liver failure presents with jaundice, coagulopathy (prolonged PT/INR), encephalopathy, and hypoglycemia — a potentially fatal complication requiring liver-supportive intensive care.
- Dengue encephalopathy and neurological manifestations: Central nervous system involvement in dengue may manifest as dengue encephalopathy (indirect, metabolic — from hepatic failure, hyponatremia, cerebral edema, or shock-related cerebral hypoperfusion), dengue encephalitis (direct viral invasion of the CNS — confirmed by dengue PCR in CSF), or specific neurological syndromes including myelitis, Guillain-Barré syndrome, acute disseminated encephalomyelitis (ADEM), cranial nerve palsies, and intracranial hemorrhage. Clinical features: seizures, altered consciousness, focal neurological deficits, meningismus, and behavioral changes. Neurological dengue complications carry high morbidity and require intensive monitoring and management.
- Dengue myocarditis and cardiac complications: Direct dengue viral infection of cardiomyocytes and immune-mediated cardiac inflammation produce dengue myocarditis — manifesting as sinus bradycardia (one of the most consistent cardiac findings, present in >50% of dengue patients during recovery), first-degree AV block, arrhythmias, reduced LVEF on echocardiography, and elevated cardiac troponin. Fulminant dengue myocarditis causing hemodynamically significant cardiac dysfunction and cardiogenic shock requires intensive cardiological support. Atrioventricular conduction abnormalities and complete heart block have been reported in severe dengue.
- Dengue acute kidney injury (AKI): Renal involvement in severe dengue ranges from proteinuria and haematuria to frank acute tubular necrosis requiring renal replacement therapy. Mechanisms include: prerenal AKI from hypovolemic shock and reduced renal perfusion; direct dengue virus-mediated tubular injury; immune complex deposition in glomeruli; rhabdomyolysis-associated myoglobinuria; and NSAID nephrotoxicity from inappropriate ibuprofen administration (a critical prescribing error in dengue, as NSAIDs are contraindicated).
6. Special Dengue Presentations
- Dengue in infants: Febrile seizures are common due to high fevers. The tourniquet test is often falsely positive in infants. Fluid overload is a particular risk due to small circulating blood volumes and difficulty assessing hydration status clinically. Early oral hydration and vigilant monitoring for tachycardia, prolonged CRT, and behavioural changes are critical. DHF in infants may present with minimal hemorrhagic manifestations but significant plasma leakage and hepatomegaly.
- Dengue in pregnancy: Dengue during pregnancy is associated with maternal complications (preterm labour, postpartum haemorrhage, placenta previa complications) and fetal complications (vertical transmission — neonatal dengue, intrauterine fetal death, low birth weight, fetal distress). Management follows the same principles as non-pregnant dengue with particular attention to fluid balance (pregnant women have altered haemodynamics), haematocrit targets, and fetal monitoring during the critical phase.
- Secondary dengue infection and ADE: A second dengue infection with a different DENV serotype triggers antibody-dependent enhancement (ADE) — pre-existing non-neutralizing heterotypic IgG antibodies from the primary infection bind the new serotype, facilitating Fcγ receptor-mediated uptake into monocytes and macrophages (dramatically increasing viral load) while simultaneously suppressing innate antiviral signaling. The resulting cytokine storm, dramatically amplified viral replication, and immune dysregulation drive the pathophysiological cascade responsible for severe dengue — making secondary infection the single strongest risk factor for DHF/DSS.
Risk Factors of Dengue Fever
Risk factors for dengue acquisition, disease severity, and poor outcomes span individual, environmental, and socio-ecological determinants:
1. Vector-Related and Environmental Risk Factors
- Residence in or travel to dengue-endemic regions: Dengue is endemic in over 128 countries across tropical and subtropical latitudes — primarily Southeast Asia, the Pacific Islands, the Caribbean, Central and South America, sub-Saharan Africa, and the Indian subcontinent. India, Brazil, Indonesia, Thailand, Mexico, and Bangladesh account for the majority of global dengue burden. Urban dwellers in these regions face the highest risk due to the peridomestic habits of Aedes aegypti. International travelers to endemic regions without prior dengue exposure are particularly vulnerable to symptomatic primary dengue infection.
- Urban living with inadequate water storage and waste management: Aedes aegypti is a highly urbanized, anthropophilic (preferring human blood meals) mosquito that breeds exclusively in clean, stagnant water in domestic and peridomestic containers — water tanks, flower pot trays, discarded tyres, bottles, clogged drains, construction water storage, and rooftop water containers. Poor urban water supply infrastructure forcing households to store water in open containers dramatically amplifies vector breeding opportunities. Inadequate solid waste management creates abundant container-based breeding habitats. Dengue risk is therefore tightly correlated with urban density, housing quality, and water and sanitation infrastructure.
- Climate and weather factors: Temperature, rainfall, and humidity profoundly influence Aedes mosquito population dynamics, biting rates, and viral replication speed. Higher ambient temperatures (25–30°C optimum) accelerate the dengue virus extrinsic incubation period within the mosquito (the time between mosquito blood meal and ability to transmit) from 12 days at 25°C to just 7 days at 30°C. Rainfall creates new breeding habitats in urban containers. El Niño Southern Oscillation (ENSO) events — producing warmer, wetter conditions in Southeast Asia and drier conditions in the Pacific — have been consistently associated with dengue epidemic cycles. Climate change is progressively expanding Aedes aegypti and albopictus geographic ranges into previously non-endemic temperate zones.
- Season: Dengue transmission is highest during and immediately after the rainy season in tropical countries — when vector breeding habitat is most abundant. In South and Southeast Asia, the dengue season corresponds to the monsoon period (June–October). Understanding the seasonal pattern in local settings enables anticipatory clinical and public health preparedness.
- Geographic expansion of Aedes albopictus: The tiger mosquito — a competent but less efficient dengue vector than aegypti — has invaded Europe (Southern France, Italy, Spain, Madeira), the United States (Eastern states), East Asia, and parts of Africa over the past three decades through global trade of used tyres (a primary larval habitat). This vector expansion is progressively bringing dengue risk to previously non-endemic temperate regions.
2. Host-Related Risk Factors for Acquiring Dengue
- Lack of immunity to circulating DENV serotype: Dengue serotype-specific immunity after natural infection is lifelong and protective against re-infection by the same serotype. However, cross-protective immunity against the other three serotypes is transient (lasting 2–9 months at most). Individuals without prior exposure to the locally circulating serotype — including dengue-naïve travelers and children in endemic settings during their first dengue season — are fully susceptible.
- Age: In hyperendemic settings (where multiple serotypes circulate simultaneously), primary dengue most commonly affects infants and young children during their initial exposures. Severe dengue (DHF/DSS) from secondary infection predominantly affects older children and young adults (ages 5–15 years in Southeast Asia) who are undergoing their second dengue infection with a heterologous serotype. However, dengue can affect all age groups, and severe dengue in adults is increasingly recognized and associated with unique clinical features including more prominent hepatic and myocardial involvement.
- Nutritional status and underlying health conditions: Malnourished children and immunocompromised individuals (HIV/AIDS, congenital immune deficiencies, organ transplant recipients) may have altered immune responses to dengue — paradoxically, some evidence suggests malnourishment may reduce the hyperimmune response driving ADE, while immunosuppression from other causes may alter dengue severity in complex and heterogeneous ways. Obesity — increasingly prevalent in dengue-endemic settings — has been associated with more severe dengue outcomes in some studies, possibly through chronic inflammation amplifying cytokine cascades.
3. Host Risk Factors for Severe Dengue (DHF/DSS)
- Secondary dengue infection (different DENV serotype) — the dominant risk factor: The probability of developing DHF/DSS is approximately 5-fold higher in secondary dengue infection compared to primary infection. ADE-amplified viral replication in monocytes/macrophages and the resulting massive cytokine storm (TNF-α, IL-6, IL-10, IFN-γ) drive the endothelial dysfunction and plasma leakage that distinguish DHF from uncomplicated dengue. DENV-2 secondary infections following primary DENV-1 are particularly associated with severe dengue. Dengue serotype sequencing studies in endemic countries confirm that secondary heterotypic infections account for the majority of DHF hospitalizations.
- DENV serotype and strain virulence: Not all dengue strains within a serotype are equally virulent. DENV-2 (Asian genotype) and DENV-3 have been associated with higher rates of severe dengue in multiple epidemic analyses. Specific viral genetic determinants in the envelope protein, NS5 polymerase, and non-structural proteins modulate viral replication efficiency, immune evasion, and endothelial permeability induction — contributing to inter-epidemic variation in dengue severity independent of host immune factors.
- Genetic host factors: HLA alleles (particularly HLA-A*0203, HLA-B*5101 are reported to modify dengue severity); polymorphisms in cytokine genes (TNF-α, IL-10, TGF-β promoter variants); polymorphisms in FcγRIIA (CD32) — the receptor mediating ADE — affect the efficiency of antibody-mediated enhanced monocyte infection; and G6PD deficiency (increasing hemolysis risk in severe dengue). Genetic ancestry (Southeast Asian vs Indian vs Latin American populations) influences dengue severity risk independent of serotype, reflecting population-level variation in immune response genes.
- Infants born to dengue-immune mothers: Maternally transferred dengue IgG antibodies in infants born to seropositive mothers can mediate ADE during primary dengue infection in the infant (typically at ages 6–12 months as maternal antibody levels wane into a sub-neutralizing range). This mechanism explains the peak incidence of DHF in infants in hyperendemic settings — they suffer ADE-enhanced primary dengue from the maternal antibody — a clinical scenario with epidemiological and vaccine safety implications.
- Pre-existing chronic diseases: Patients with diabetes mellitus, hypertension, cardiovascular disease, obesity, asthma, or chronic kidney disease demonstrate higher rates of severe dengue, prolonged hospitalization, more frequent organ dysfunction, and greater mortality compared to patients without comorbidities. These conditions amplify the inflammatory and hemodynamic perturbations of severe dengue and reduce physiological reserve during dengue shock.
Diagnosis of Dengue Fever
Dengue diagnosis integrates clinical assessment (fever, retro-orbital pain, myalgia, rash, tourniquet test, warning signs), epidemiological context (travel to/residence in endemic area, dengue season), and laboratory confirmation. The appropriate diagnostic test depends on the day of illness — virological tests (NS1, PCR) are positive during early viremia; serological tests (IgM/IgG) become positive after the first week.
1. Clinical Diagnosis
- WHO clinical case definition (probable dengue): Fever plus residence in or travel to endemic area within 14 days PLUS two or more of: nausea/vomiting; rash; aches and pains (myalgia/arthralgia); positive tourniquet test; leukopenia (WBC ≤5,000/mm³); any warning sign. Clinical diagnosis is sufficient to initiate management in resource-limited or outbreak settings; laboratory confirmation adds specificity and guides serotype surveillance.
- Tourniquet test (Rumple-Leede test): A practical, inexpensive, bedside test for capillary fragility: inflate BP cuff to midpoint between systolic and diastolic (or to 100 mmHg) for 5 minutes; count petechiae in a 1-inch square area in the antecubital fossa; positive test = ≥10 petechiae/square inch. Sensitivity for dengue approximately 70–80%; specificity limited (can be positive in other thrombocytopenic states). Widely used in primary care and outpatient settings in endemic countries as the initial screening test.
- Haematocrit monitoring — the cornerstone of dengue clinical management: Serial haematocrit measurements (every 6–8 hours during the febrile phase; every 4–6 hours during the critical phase) are essential in all hospitalized dengue patients to detect hemoconcentration. A haematocrit rise of ≥20% over baseline or above age-adjusted upper normal (adult male Hct >50%; female >46%) indicates plasma leakage — triggering the decision to initiate IV fluid therapy in DHF. Conversely, a falling haematocrit without clinical improvement suggests internal bleeding.
2. Laboratory Diagnosis — Virological Tests
- NS1 Antigen RDT / ELISA : Non-structural protein 1 — secreted by dengue-infected cells; detectable Days 1–9 of illness. RDT (rapid diagnostic test): point-of-care, 15–30 min, sensitivity 70–90% (Day 1–5), >95% specificity. ELISA NS1: higher sensitivity (90–95% Day 1–4). Falls rapidly after Day 5. Negative NS1 does NOT exclude dengue if tested after Day 5.
- RT-PCR (Dengue Molecular Diagnosis) : Reverse-transcriptase PCR detecting DENV genome RNA in serum/plasma. Gold standard for virological diagnosis — highest sensitivity Days 1–5 (sensitivity >95%). Also provides serotype identification — critical for epidemiological surveillance. Multiplex dengue/Zika/chikungunya RT-PCR panels available for co-circulation differential diagnosis. Requires specialized laboratory, not point-of-care.
- Virus Isolation (Cell Culture) : Isolation of dengue virus in Vero cells or C6/36 cells — reference standard for epidemiological research and vaccine development. Requires BSL-2/3 facility, 7–14 days; impractical for clinical diagnosis. Used for strain characterization, phylogenetic analysis, and monitoring of serotype circulation patterns.
3. Laboratory Diagnosis — Serological Tests
- IgM ELISA (MAC-ELISA) : Dengue IgM becomes detectable ~Day 5–6 (primary) or Day 4 (secondary). Peaks 2 weeks post-illness; persists 2–3 months. Single IgM positive: presumptive diagnosis. Sensitivity: Days 5–14 approximately 90%. Cross-reactivity with other flaviviruses (Zika, Japanese encephalitis, West Nile) limits specificity.
- IgG ELISA / Primary vs Secondary : Low/absent IgG with positive IgM: primary dengue infection. High IgG (rising rapidly) with positive IgM: secondary dengue. IgG/IgM ratio >1.2 by HI assay suggests secondary infection (stronger DHF risk). IgG persists lifelong — indicates prior dengue exposure. Avidity testing distinguishes acute from past infection.
- NS1 + IgM Combo RDT :Combined NS1 antigen + IgM antibody rapid test on a single lateral-flow platform — maximizes diagnostic sensitivity across all days of illness (Days 1–14) within a single test. Widely used in clinical settings in endemic countries. Overall sensitivity ~92%, specificity ~95% compared to PCR-confirmed dengue.
4. Haematological and Biochemical Investigations
- Complete blood count (CBC) with differential: The most important baseline and monitoring investigation in dengue. Characteristic findings: leukopenia (WBC ≤5,000/mm³; lymphocyte predominance with atypical lymphocytes) — typically present by day 3 of fever; progressive thrombocytopenia (platelet count ≤100,000/mm³ by day 5–7 in DHF; nadir <20,000/mm³ in severe DHF); rising haematocrit (hemoconcentration ≥20% in DHF). Serial CBC every 12–24 hours in stable dengue; every 4–6 hours in warning signs or DHF.
- Platelet count — critical monitoring parameter: The rate of platelet fall and the nadir platelet count are key parameters guiding clinical decisions. A platelet count falling >10,000/mm³ per day combined with a rising haematocrit signals imminent critical-phase transition. Spontaneous bleeding risk increases significantly at platelet counts <20,000/mm³; prophylactic platelet transfusion is considered at <10,000–20,000/mm³ in patients with active bleeding or planned invasive procedures.
- Liver function tests (ALT, AST, bilirubin, albumin): Elevated ALT and AST (hepatic transaminases) in virtually all dengue cases — AST characteristically rises earlier and to higher levels than ALT (unlike typical viral hepatitis). ALT/AST >1000 IU/L constitutes severe dengue. Hypoalbuminaemia reflects liver synthetic dysfunction and contributes to plasma oncotic pressure reduction and exacerbated plasma leakage. Conjugated hyperbilirubinemia in dengue hepatitis.
- Serum electrolytes and renal function: Hyponatremia (dilutional, from increased ADH in febrile illness and from plasma leakage replacement with hypotonic fluids) is common and may contribute to cerebral edema and seizures. Renal function tests (urea, creatinine, eGFR) for early detection of dengue AKI. Urinalysis for proteinuria, hematuria, and casts indicating glomerular or tubular involvement.
- Serum proteins and albumin: Declining serum albumin and total protein levels provide early evidence of protein-containing plasma leakage from the intravascular compartment. Hypoproteinaemia combined with haemoconcentration is pathognomonic of dengue plasma leakage syndrome.
- Coagulation studies (PT, aPTT, fibrinogen, D-dimer): In severe dengue with hepatic failure or DIC-like coagulopathy: prolonged PT/aPTT, decreased fibrinogen, elevated D-dimer, and decreased clotting factors. These parameters guide blood product support requirements (fresh frozen plasma, cryoprecipitate). Coagulopathy superimposed on thrombocytopenia creates a compounded hemorrhagic risk.
- C-reactive protein (CRP) and procalcitonin: CRP is typically mildly elevated in dengue (in contrast to high elevation in bacterial sepsis); procalcitonin is usually low in uncomplicated dengue. These markers help differentiate dengue from bacterial infections or superimposed bacterial sepsis in dengue patients who remain febrile and deteriorate despite apparently typical dengue clinical course.
5. Imaging in Dengue
- Chest X-ray: Detects pleural effusions (typically right-sided initially, then bilateral in severe dengue) — appearing as basal haziness or blunting of costophrenic angles. Interstitial pulmonary oedema or dengue pneumonitis may appear as diffuse bilateral interstitial infiltrates. The appearance of pleural effusions on CXR in a dengue patient confirms plasma leakage and indicates DHF even in the absence of overt haemoconcentration if haematocrit is diluted by early IV fluid administration.
- Abdominal ultrasonography: The most sensitive imaging tool for detecting subclinical plasma leakage in dengue — highly recommended in all patients with warning signs and in suspected DHF. Ultrasound detects: ascites (free peritoneal fluid, typically echogenic leaked plasma); bilateral pleural effusions; gallbladder wall thickening and oedema (a characteristic and early sonographic finding in dengue, resulting from localised plasma leakage around the gallbladder — gallbladder wall thickness >3 mm is suggestive); hepatomegaly and splenomegaly; pancreatic oedema; and perinephric fluid.
- Echocardiography: For dengue myocarditis evaluation (reduced LVEF, pericardial effusion, regional wall motion abnormalities), assessment of volume status in fluid management decisions (inferior vena cava collapsibility index for volume responsiveness), and diagnosis of dengue-related hemodynamic compromise in the ICU.
- CT brain / MRI brain: Reserved for dengue patients with neurological manifestations — seizures, altered consciousness, focal deficits. CT identifies intracranial hemorrhage, cerebral edema, or herniation. MRI better characterizes dengue encephalitis (T2/FLAIR hyperintensities), ADEM, myelitis, and subtle edematous changes.
Complications of Dengue Fever
While the majority of dengue infections are self-limiting, a significant subset — particularly secondary infections and those in high-risk groups — develops potentially fatal complications spanning multiple organ systems:
A. Circulatory Complications
- Dengue Shock Syndrome (DSS): The leading cause of dengue-associated death, DSS results from massive plasma extravasation into serous cavities and the interstitium through dengue-damaged capillary endothelium. The consequent intravascular volume depletion produces hypovolemic shock, with clinical features of cold clammy extremities, tachycardia, narrow pulse pressure (≤20 mmHg — a critical early sign reflecting reduced stroke volume), falling blood pressure, prolonged capillary refill time, oliguria, and metabolic acidosis. Without prompt IV fluid resuscitation, DSS progresses rapidly to organ failure and death. Mortality with appropriate management at experienced dengue centres is <1%; without management, mortality exceeds 10–20%.
- Fluid overload from over-enthusiastic IV fluid resuscitation: A critical and frequently encountered complication of dengue management — paradoxically arising from the treatment itself. During the recovery phase (days 7–10), reabsorption of the leaked plasma back into the intravascular space creates an abrupt rise in circulating blood volume. If IV fluids are not stopped or significantly reduced as the patient transitions into recovery (heralded by improving clinical status, falling haematocrit, rising platelet count, onset of diuresis), fluid overload develops — causing pulmonary oedema, respiratory failure, hypertension, and cardiac strain. This is why dengue fluid management requires active, protocolised reassessment at every phase.
B. Hemorrhagic Complications
- Gastrointestinal hemorrhage: The most clinically significant hemorrhagic complication — arising from thrombocytopenia, platelet dysfunction, coagulopathy (dengue-associated liver synthetic failure), mucosal erosion from dengue-induced GI inflammation, and mucosal ischaemia from DSS. Manifest as hematemesis (vomiting blood, fresh or "coffee-ground"), melena (black, tarry, foul-smelling stools from upper GI bleeding), or frank hematochezia (bright red rectal bleeding). Massive GI hemorrhage may cause acute exsanguinating blood loss requiring emergency blood transfusion and platelet support.
- Intracranial hemorrhage: A rare but frequently fatal complication — subarachnoid hemorrhage, subdural hemorrhage, intracerebral hemorrhage, and intraventricular hemorrhage — arising from severe thrombocytopenia (<10,000/mm³), coagulopathy, and cerebrovascular fragility. Presents with sudden severe headache, altered consciousness, focal neurological deficits, seizures, or decerebrate posturing. CT brain confirms the diagnosis; emergency neurosurgical consultation and blood product support are required.
- Pulmonary hemorrhage and hemoptysis: Diffuse alveolar hemorrhage in severe dengue — manifesting as hemoptysis, acute respiratory failure with bilateral alveolar opacities on CXR/CT, and falling haematocrit — requires ICU-level respiratory support and platelet transfusion.
C. Organ Failure Complications
- Acute liver failure: Dengue-associated fulminant hepatic failure is a rare but potentially fatal complication, characterized by massive hepatocyte death from direct dengue cytopathic injury, hypoxic hepatitis from DSS-related hepatic ischaemia, and immune-mediated hepatocellular damage. Features: acute jaundice, profoundly elevated transaminases (ALT/AST >5000 IU/L), coagulopathy (INR >1.5), hypoglycaemia, hyperammonaemia, and hepatic encephalopathy. Management follows acute liver failure protocols: N-acetylcysteine, glucose supplementation, lactulose for encephalopathy, FFP/vitamin K for coagulopathy, and liver transplant evaluation in selected cases.
- Dengue-associated haemophagocytic lymphohistiocytosis (HLH): A rare, severe complication of dengue characterized by pathological macrophage activation and haemophagocytosis in the bone marrow, liver, and spleen. Clinical features: persistent fever beyond day 10, severe cytopenias (pancytopenia), very high ferritin (>500 µg/L), splenomegaly, and coagulopathy. Dengue HLH carries high mortality; treatment includes IVIG, corticosteroids (dexamethasone), and cyclosporine A in refractory cases.
- Acute kidney injury: Ranging from reversible pre-renal AKI (resolved with fluid resuscitation) to intrinsic AKI from direct viral tubular injury, immune complex glomerulonephritis, myoglobinuria from rhabdomyolysis, or NSAID-induced nephrotoxicity. Renal replacement therapy (haemodialysis or haemofiltration) may be required in severe cases.
- Expanded dengue syndrome: Rare but increasingly recognized organ manifestations including dengue uveitis (anterior or posterior uveitis with visual impairment), orchitis, oophoritis, myositis, pancreatitis, and dengue-associated haemolytic uraemic syndrome (HUS) — collectively forming the spectrum of "expanded dengue syndrome" representing unusual dengue manifestations requiring specific specialist evaluation.
D. Post-Dengue Complications
- Post-dengue fatigue syndrome: A well-documented post-infectious syndrome affecting approximately 30–40% of dengue patients following apparent clinical recovery — characterized by persistent fatigue, weakness, myalgia, cognitive impairment ("brain fog"), depression, and reduced functional capacity lasting weeks to months. The mechanism overlaps with post-viral fatigue syndromes seen after other viral infections; management is supportive with gradual graded rehabilitation. Most patients fully recover within 2–6 months.
- Post-dengue uveitis: Dengue-associated uveitis may develop during the acute illness or weeks after apparent recovery — presenting as eye redness, photophobia, blurred vision, and floaters. Both anterior uveitis and multifocal choroiditis have been described. Dengue uveitis requires prompt ophthalmological evaluation and topical corticosteroid therapy to prevent permanent visual impairment.
Treatment of Dengue Fever
There is no approved specific antiviral therapy for dengue. Treatment is entirely supportive and symptomatic, guided by meticulous clinical and laboratory monitoring. The WHO guidelines recommend stratifying management based on the clinical category (dengue without warning signs; dengue with warning signs; severe dengue) and disease phase (febrile, critical, recovery).
A. Dengue Without Warning Signs — Outpatient Management
- Oral fluid hydration — the single most important intervention: Adequate hydration is the cornerstone of dengue outpatient management, replacing fluid losses from fever, diaphoresis, reduced oral intake, and subclinical plasma leakage. WHO recommends a minimum of 5 glasses (250 mL each) of fluid per day for adults — including water, oral rehydration salts (ORS), coconut water, fruit juices without pulp, and soups. ORS provides an isotonic glucose-electrolyte solution that is ideal for dengue hydration. Patients should be explicitly instructed on the signs requiring immediate hospital return (warning signs).
- Paracetamol (acetaminophen) for fever and pain: The ONLY safe antipyretic and analgesic in dengue. Standard dosing: 500–1000 mg every 6 hours (adults); 10–15 mg/kg/dose in children (maximum 4 doses per 24 hours). Paracetamol is preferred over NSAIDs because it does not inhibit platelet function, does not cause gastric erosion or GI bleeding, and does not impair renal prostaglandin synthesis. High-dose paracetamol (>4 g/day in adults) should be avoided given the background risk of dengue hepatotoxicity.
- Rest and activity restriction: Patients should rest during the acute febrile phase to reduce metabolic demands, prevent orthostatic hypotension from rapid temperature changes, and minimise risk of bleeding from trauma in thrombocytopenic patients. Physical activity is gradually resumed after the critical phase has safely passed and the platelet count is recovering.
- Monitoring and warning sign education: All outpatient dengue patients and their caregivers must receive clear, explicit education regarding the WHO warning signs that require immediate emergency department return: abdominal pain, persistent vomiting, bleeding from any site, difficulty breathing, restlessness or lethargy, pallor, and passage of dark urine or black stools. A clinical review visit should be scheduled for days 4–6 of illness — the critical phase window — regardless of clinical status.
- Daily CBC monitoring (platelet count and haematocrit): In all dengue patients, daily CBC during the febrile phase (particularly from day 3 onwards) identifies early thrombocytopenia and haemoconcentration. Serial monitoring allows anticipatory hospital admission before clinical deterioration, when IV fluid therapy can be initiated in a controlled, proactive manner rather than as an emergency resuscitation.
B. Dengue With Warning Signs — Hospital-Based Management
Intravenous fluid therapy in DHF must be precisely calibrated — neither insufficient (risking shock) nor excessive (risking fluid overload in recovery). The WHO-recommended IV fluid for dengue is isotonic crystalloid: Normal Saline (0.9% NaCl), Hartmann's solution (Lactated Ringer's), or 5% Dextrose in 0.45% NaCl. Colloids (dextran-40, gelatin solutions, 6% HES) are reserved for DSS refractory to crystalloids. Dextrose 5% alone (hypotonic) is inappropriate and worsens hyponatraemia. Blood pressure, pulse pressure, peripheral perfusion, urine output (target ≥0.5–1 mL/kg/hour), and serial haematocrit guide fluid rate adjustment every 1–2 hours during the critical phase.
- IV crystalloid fluid therapy — titrated to haematocrit and clinical response: Initial IV fluid rate for dengue with warning signs: 5–7 mL/kg/hour of crystalloid for 1–2 hours, then reduce to 3–5 mL/kg/hour for 2–4 hours, then 2–3 mL/kg/hour if improving — reassessed by repeated haematocrit. If haematocrit continues to rise or clinical status deteriorates: fluid bolus 10–20 mL/kg over 15–30 minutes (colloid preferred in escalated deterioration). If haematocrit falls rapidly (internal bleeding — not improvement): reassess for occult haemorrhage.
- Electrolyte correction: Hyponatraemia (Na <130 mmol/L) is corrected gradually with isotonic saline (not hypertonic saline unless severe symptomatic hyponatraemia with seizures). Hypokalaemia from inadequate intake and dengue-associated renal losses requires potassium supplementation (IV or oral). Metabolic acidosis from lactic acidosis in DSS is corrected by restoring perfusion with adequate fluid resuscitation — sodium bicarbonate is not routinely recommended.
- Platelet transfusion — narrow, evidence-based indications: Prophylactic platelet transfusion for dengue thrombocytopenia without bleeding is NOT routinely recommended (no evidence of benefit; risk of volume overload and transfusion reactions). Indications: active significant bleeding with platelet count <50,000/mm³ (therapeutic transfusion); platelet count <10,000–20,000/mm³ in a patient with warning signs of bleeding or planned emergency surgery. Fresh frozen plasma (FFP) and cryoprecipitate are given for documented coagulopathy with active bleeding.
- Blood transfusion: Packed red blood cells for dengue patients with significant GI haemorrhage, haemoglobin <7 g/dL with active bleeding, or evidence of haemodynamic compromise from haemorrhage. Avoid blood transfusion in stable patients with low haematocrit from haemodilution during fluid resuscitation (distinguish from true haemorrhagic anaemia).
C. Severe Dengue (DSS) — ICU Management
- Emergency fluid resuscitation: Immediate IV fluid bolus: 10–20 mL/kg of isotonic crystalloid over 15–20 minutes. If no improvement within 30 minutes: repeat fluid bolus (colloid preferred — dextran-40 or 6% HES 10 mL/kg if available) AND reassess for occult haemorrhage. Continuous monitoring of vital signs every 15–30 minutes; consider arterial line and CVP monitoring in refractory shock.
- Oxygen therapy and ventilatory support: High-flow oxygen via face mask or reservoir mask for dengue patients with respiratory distress, pulmonary oedema, or SpO₂ <94%. Non-invasive positive pressure ventilation (BiPAP/CPAP) for cardiogenic pulmonary oedema. Mechanical ventilation (endotracheal intubation) for severe respiratory failure or cerebral complications with reduced GCS — acknowledging that intubation of a dengue patient with severe thrombocytopenia and coagulopathy carries significant procedural haemorrhagic risk.
- Inotropic support: Dopamine or noradrenaline (norepinephrine) infusion for haemodynamically unstable DSS refractory to adequate fluid resuscitation — particularly when myocardial depression from dengue myocarditis contributes to haemodynamic instability. Inotropes are supplementary to, not substitutes for, adequate volume resuscitation.
- Management of bleeding complications: GI haemorrhage: IV proton pump inhibitor (pantoprazole or omeprazole), nil by mouth, endoscopic evaluation when platelet count allows and haemodynamic stability permits, blood transfusion. Intracranial haemorrhage: emergent platelet transfusion to maintain count >50,000/mm³, FFP for coagulopathy, neurosurgical consultation. Dengue HLH: IVIG 2 g/kg over 5 days, dexamethasone 10 mg/m²/day, cyclosporine A in refractory cases.
Dengue prevention is an integrated, multi-level challenge requiring individual-level personal protection, community-level vector control, health system surveillance and preparedness, and — increasingly — vaccine-based immunity strategies. The WHO's dengue prevention framework integrates all four pillars of its Global Vector Control Response (GVCR) 2017–2030: strengthening vector surveillance; environmental management; biological control; and evidence-based insecticidal interventions. 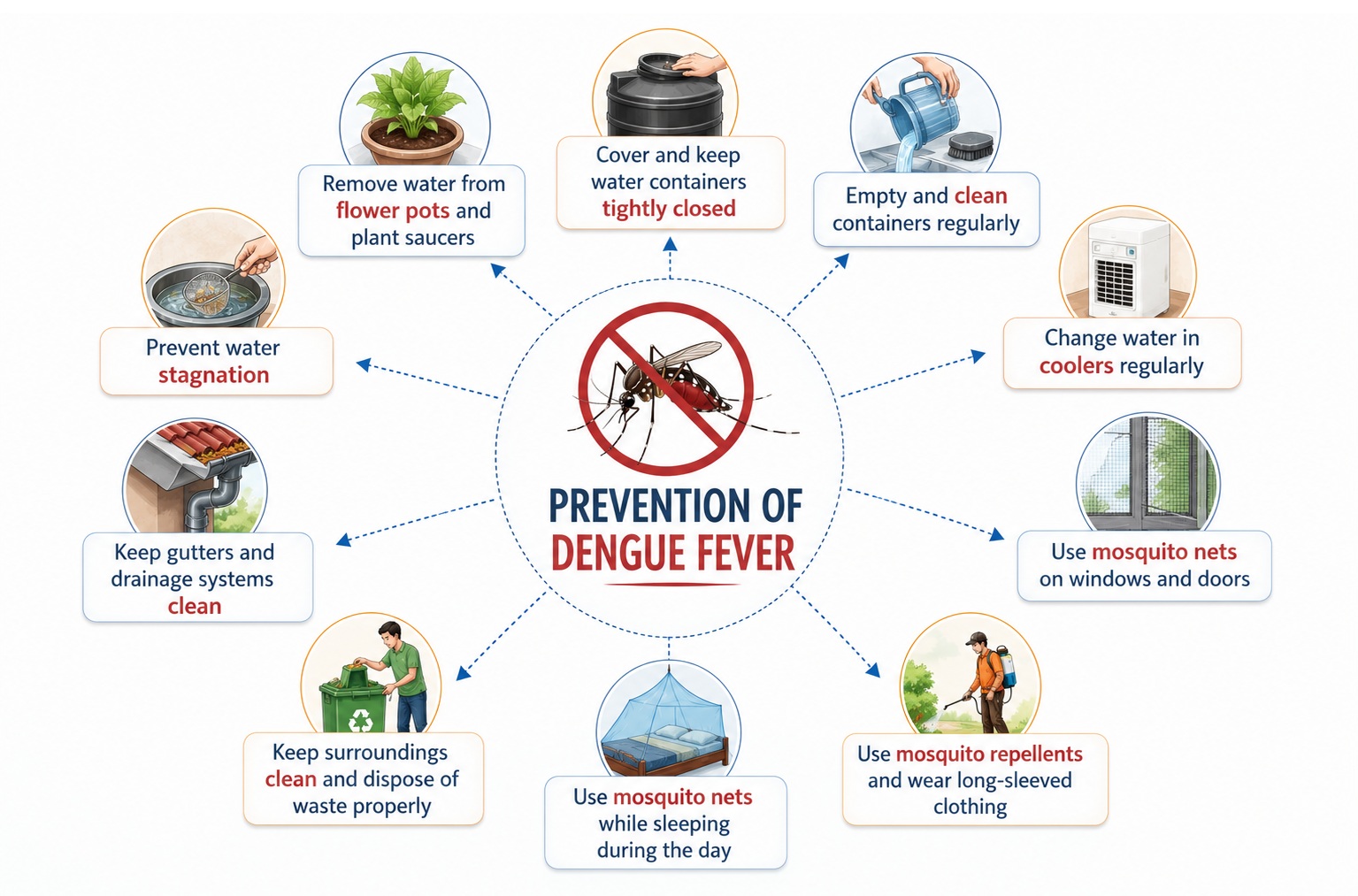
A. Individual and Household Protection
- Personal protective measures against Aedes mosquito bites: Aedes aegypti is a day-biting mosquito (peak biting activity at dawn and dusk, but active throughout the day) — unlike malaria vectors (night-biting). Therefore, dengue prevention requires daytime protection measures: DEET-based insect repellents (N,N-Diethyl-meta-toluamide, 20–50% concentration) applied to all exposed skin; Picaridin (Icaridin, 20%); IR3535 repellents; and oil of lemon eucalyptus (OLE) — all effective against Aedes when applied correctly and reapplied every 4–6 hours. Long-sleeved clothing, long trousers, and light-coloured clothing (mosquitoes are attracted to dark colours) provide physical protection.
- Source reduction — eliminating Aedes breeding sites: The most impactful and durable household dengue prevention measure — removing, covering, or treating all potential water-holding containers that serve as Aedes breeding habitats. Weekly household inspection and action on: emptying and inverting all water storage containers weekly (breaking the Aedes egg-to-adult cycle, which requires approximately 7 days); covering water storage tanks with tight-fitting lids; changing water in flower pot trays and pet water dishes weekly; removing discarded tyres, tin cans, and bottles; cleaning and flushing blocked drains; and treating ornamental water features with Bacillus thuringiensis israelensis (Bti) — a safe biological larvicide.
- Indoor and outdoor insecticides: Insecticide-treated mosquito nets (ITNs) used during daytime naps and by young children and infants; indoor residual spraying of permethrins on walls and fabric surfaces; electric mosquito repellent devices (vapourizers, coils); mosquito screens on windows and doors to prevent indoor mosquito access; aerosol insecticide sprays in indoor resting areas.
- Travel precautions: Travellers to dengue-endemic regions should register travel health visits, receive dengue risk information and repellent prescriptions pre-departure, comply diligently with personal protection measures throughout their stay, seek medical attention promptly if febrile within 14 days of return, and inform healthcare providers of their travel history (dengue diagnosis is frequently missed or delayed in non-endemic countries due to low clinical awareness).
B. Community and Environmental Vector Control
- Community-based source reduction programmes: Systematic government-organised or community-led source reduction campaigns — conducted weekly during dengue season by community health workers, schoolchildren (student vector surveillance brigades), and neighbourhood voluntary teams — achieve substantially greater elimination of Aedes breeding sites than individually motivated household action alone. Community engagement, social mobilisation, and health education are essential components of sustained vector control effectiveness.
- Larval control — Bacillus thuringiensis israelensis (Bti): Bti is a naturally occurring soil bacterium that produces Cry-type protein crystals selectively lethal to mosquito larvae upon ingestion, with no toxicity to humans, animals, fish, or non-target insects. Bti temephos granules applied to water storage containers, ornamental ponds, and drains achieve >95% larval mortality within 24 hours. It is the WHO-recommended biological larvicide for community dengue control and does not develop resistance under field conditions, unlike chemical larvicides.
- Space spraying (fogging) with adulticide insecticides: Ultra-low volume (ULV) space spraying of synthetic pyrethroids (deltamethrin, lambda-cyhalothrin) or organophosphates (malathion) during dengue outbreaks kills adult flying mosquitoes in the target area. However, fogging provides only temporary reduction in adult vector populations (hours to days), does not reach resting mosquitoes in indoor areas, kills beneficial pollinator insects and natural mosquito predators, and is associated with emerging pyrethroid resistance in Aedes populations. WHO recommends fogging only as a complementary emergency measure during active outbreaks combined with sustained source reduction — not as a standalone vector control strategy.
- Environmental management and urban planning: Improving urban water supply infrastructure to eliminate the need for household water storage; improving solid waste collection to remove container habitats; engineering urban drainage systems to prevent stagnant water accumulation; eliminating peridomestic containers through bylaws requiring property owners to inspect and remove containers; and designing urban green spaces to eliminate container-type microhabitats. These structural environmental management interventions address the root causes of Aedes vector proliferation with the greatest long-term public health impact.
C. Innovative Biological Vector Control Strategies
- Wolbachia-infected Aedes aegypti release (World Mosquito Programme): Wolbachia is an intracellular bacterium naturally found in approximately 60% of insect species but not in Aedes aegypti. When Wolbachia (specifically the wMel strain) is introduced into Aedes aegypti, it profoundly reduces the mosquito's ability to replicate dengue virus, Zika virus, and chikungunya virus — through multiple mechanisms including competition for cellular resources, antiviral immune activation, and shortened mosquito lifespan. Critically, Wolbachia-infected mosquitoes spread through natural mosquito populations via cytoplasmic incompatibility (non-Wolbachia females cannot successfully reproduce with Wolbachia males, creating selective pressure favouring spread of Wolbachia-infected lineages). Field trials in Yogyakarta, Indonesia (AWED trial) demonstrated a 77% reduction in dengue incidence and 86% reduction in dengue hospitalizations in Wolbachia release areas compared to controls — the most compelling dengue prevention data published to date. The World Mosquito Programme is expanding releases to multiple dengue-endemic countries.
- Sterile Insect Technique (SIT) and genetic control: Release of sterile male Aedes aegypti (irradiated to render their sperm non-viable) into the environment to compete with wild males for female mating — reducing the proportion of fertile matings and progressively suppressing vector populations. Oxitec's OX513A (GM male mosquitoes carrying a dominant lethal gene) and OX4319 (female-lethal) constructs have been trialled in Brazil, Cayman Islands, and the US with significant local vector suppression. These approaches require sustained release programs to maintain population suppression.
D. Dengue Vaccines
- Dengvaxia (CYD-TDV, Sanofi Pasteur) — First Licensed Dengue Vaccine: A live-attenuated chimeric tetravalent dengue vaccine based on a yellow fever 17D backbone expressing dengue envelope and pre-membrane proteins for all four DENV serotypes. Approved in 20+ countries for individuals aged 9–45 years in endemic settings. The critical Dengvaxia safety revelation (2017): in dengue-naïve recipients (individuals without prior dengue infection), Dengvaxia acts as a "virtual first dengue infection," sensitizing seronegative vaccinees to more severe dengue upon their first natural dengue infection post-vaccination — the ADE mechanism applied to vaccine-primed naive individuals. WHO and regulatory agencies therefore mandate pre-vaccination dengue serostatus screening (proof of prior dengue infection) before Dengvaxia administration; it is only recommended for confirmed seropositive individuals. Efficacy in seropositive recipients: approximately 78% against symptomatic dengue and 93% against hospitalisation after 3 doses.
- Qdenga (TAK-003, Takeda) — New Generation Tetravalent Dengue Vaccine: A live-attenuated tetravalent dengue vaccine using a DENV-2 backbone to express all four dengue serotypes. Approved by EMA (2022) for individuals aged 4–60 years in endemic settings. The key advantage over Dengvaxia: TAK-003 does not appear to sensitize seronegative recipients to enhanced dengue severity — in the TIDES Phase III trial, TAK-003 demonstrated 61.2% overall efficacy against symptomatic dengue and 84.1% efficacy against dengue hospitalisation over 4.5 years of follow-up, including significant efficacy in seronegative recipients. This makes TAK-003 suitable for vaccination programs without mandatory pre-vaccination serology screening, dramatically simplifying national immunisation program implementation. Two doses 3 months apart; approved in multiple Asian and Latin American countries.
- Dengue surveillance and outbreak preparedness: Sentinel hospital-based dengue surveillance, serotype monitoring, entomological surveillance (Breteau index, container index), and epidemiological early warning systems enable anticipatory public health responses (pre-emptive vector control intensification, healthcare system preparedness, public health communication) that reduce outbreak amplitude and severity. The WHO Dengue ALERT (Automated Local Dengue Early Reporting Tool) and national IHR reporting obligations form the international framework for dengue outbreak detection and response.
Common FAQs on Dengue Fever
Bibliography on Dengue Fever
- World Health Organization. Dengue and Severe Dengue — Key Facts. WHO Fact Sheet. Updated March 2023. Geneva: WHO.
- World Health Organization. Dengue: Guidelines for Diagnosis, Treatment, Prevention and Control — New Edition. WHO/HTM/NTD/DEN/2009.1. Geneva: WHO Press, 2009.
- Bhatt S, Gething PW, Brady OJ, et al. The global distribution and burden of dengue. Nature. 2013;496(7446):504–507.
- Halstead SB. Dengue. Lancet. 2007;370(9599):1644–1652. [Comprehensive review of dengue pathophysiology and ADE]
- Hadinegoro SR, Arredondo-García JL, Capeding MR, et al. Efficacy and Long-Term Safety of a Dengue Vaccine in Regions of Endemic Disease. New England Journal of Medicine. 2015;373(13):1195–1206. [CYD14/CYD15 — Dengvaxia Phase III]
- Sridhar S, Luedtke A, Langevin E, et al. Effect of Dengue Serostatus on Dengue Vaccine Safety and Efficacy. New England Journal of Medicine. 2018;379(4):327–340. [Dengvaxia seronegative risk — critical safety study]
- Rivera L, Biswal S, Sáez-Llorens X, et al. Three-Year Efficacy and Safety of Takeda's Dengue Vaccine Candidate (TAK-003). Clinical Infectious Diseases. 2022;75(1):107–117. [TIDES TAK-003 — Qdenga]
- Utarini A, Indriani C, Ahmad RA, et al. Efficacy of Wolbachia-Infected Mosquito Deployments for the Control of Dengue. New England Journal of Medicine. 2021;384(23):2177–2186. [AWED Trial — Wolbachia RCT]
- Simmons CP, Farrar JJ, Nguyen VVC, Wills B. Dengue. New England Journal of Medicine. 2012;366(15):1423–1432. [Comprehensive clinical review]
- Gubler DJ. Dengue and dengue hemorrhagic fever. Clinical Microbiology Reviews. 1998;11(3):480–496. [Historical epidemiology and pathogenesis]
- WHO Technical Expert Group on Dengue. Evidence to recommendation framework for the use of dengue vaccines. WHO Strategic Advisory Group of Experts on Immunisation (SAGE), 2018.
- Murhekar MV, Kanagasabai K, Shete V, et al. Dengue burden in India: recent trends and importance of reporting. WHO South-East Asia Journal of Public Health. 2019;8(1):14–20.
- Tissera H, Rathore AP, Kanakaratne N, et al. Serological and molecular dengue diagnostics: challenges and opportunities. Expert Review of Anti-infective Therapy. 2018;16(6):471–481.
- Brady OJ, Gething PW, Bhatt S, et al. Refining the Global Spatial Limits of Dengue Virus Transmission by Evidence-Based Consensus. PLOS Neglected Tropical Diseases. 2012;6(8):e1760.
- Harrison's Principles of Internal Medicine, 21st ed. Editors: Jameson JL, Fauci AS, Kasper DL, et al. McGraw-Hill Education. Chapter: Dengue and Other Arboviral Infections.