











Coronary Artery Disease (CAD) – Sign and Symptoms, Risk Factors, Diagnosis, Complications, Treatment and Prevention
Coronary Artery Disease (CAD) is a chronic atherosclerotic cardiovascular disorder characterized by the narrowing or obstruction of the coronary arteries due to the accumulation of lipid-rich plaques within the arterial wall. This process leads to reduced myocardial perfusion and oxygen supply, resulting in myocardial ischemia. Coronary Artery Disease (CAD) — also termed ischemic heart disease (IHD), coronary heart disease (CHD), or atherosclerotic cardiovascular disease (ASCVD) — is the single most common cause of death globally, responsible for approximately 7.4 million deaths annually and affecting an estimated 523 million individuals worldwide. It encompasses a pathological spectrum of conditions arising from the progressive narrowing or occlusion of the coronary arteries — the vessels that supply oxygenated blood to the myocardium — most commonly through the process of atherosclerosis, which involves the accumulation of lipid-laden plaques within the intimal layer of the coronary arterial wall. Atherosclerosis is fundamentally an inflammatory disease: endothelial dysfunction allows modified low-density lipoprotein (LDL) particles to penetrate the intima, where they are oxidized and ingested by macrophages forming foam cells, which accumulate to form fatty streaks that progress over decades to fibrous plaques capable of restricting coronary blood flow or, upon rupture, triggering acute coronary thrombosis.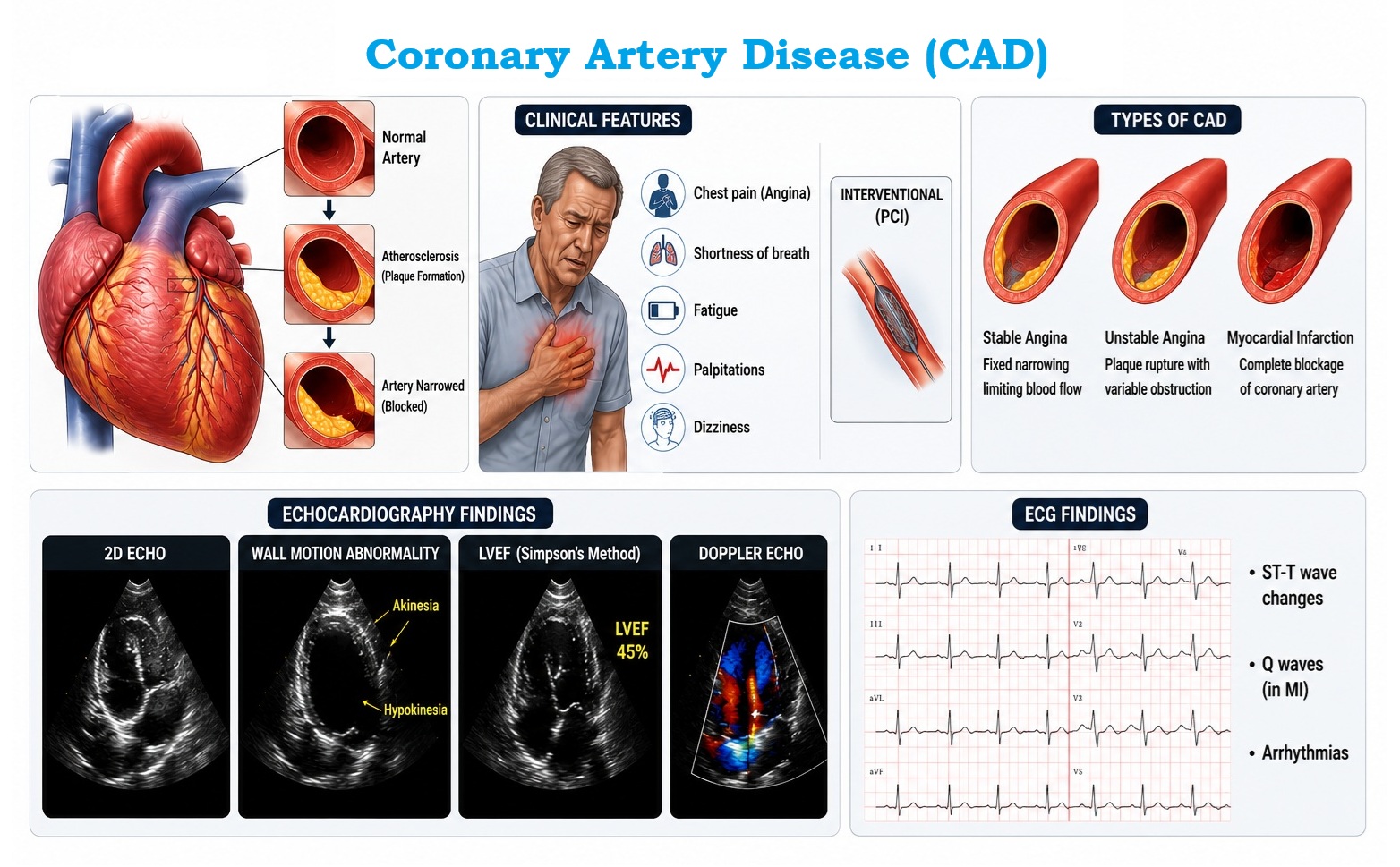
CAD presents across a broad clinical spectrum. Chronic coronary syndrome (CCS) — formerly "stable CAD" — encompasses stable angina pectoris, silent myocardial ischemia, ischemic cardiomyopathy, and coronary artery spasm, where symptoms are predictable and triggered by exertion or emotional stress when myocardial oxygen demand exceeds the fixed supply through a stenosed artery. Acute coronary syndromes (ACS) arise when atherosclerotic plaque rupture or erosion triggers acute thrombosis, producing the spectrum of unstable angina (UA), non-ST-elevation myocardial infarction (NSTEMI), and ST-elevation myocardial infarction (STEMI) — medical emergencies that mandate immediate revascularization to limit myocardial necrosis and prevent death. The extent of myocardial damage in ACS is powerfully time-dependent: "time is muscle" reflects the exponential loss of viable cardiomyocytes with every minute of unrestored coronary flow.
The risk factors for CAD are among the most thoroughly characterized in all of medicine, spanning non-modifiable factors (age, sex, family history, genetics) and highly modifiable factors (dyslipidemia, hypertension, diabetes mellitus, smoking, obesity, physical inactivity, unhealthy diet, and psychosocial stress). The Framingham Heart Study — a landmark longitudinal cohort study initiated in 1948 — established the quantitative relationships between these risk factors and CAD incidence that underpin modern cardiovascular risk prediction models. Contemporary evidence-based management integrates lifestyle modification, optimal medical therapy (statins, antiplatelet agents, ACE inhibitors, beta-blockers), and where indicated, coronary revascularization — percutaneous coronary intervention (PCI) with drug-eluting stents or coronary artery bypass grafting (CABG). Landmark trials including ISCHEMIA, COURAGE, SYNTAX, and EXCEL have refined indications for revascularization versus optimal medical therapy in CCS. The global burden of CAD demands both individual-level risk factor management and population-level primary prevention strategies targeting the societal determinants of cardiovascular disease.
This comprehensive article provides a detailed, evidence-based review of CAD pathophysiology, classification, signs and symptoms, risk factors, diagnostic evaluation, complications, treatment strategies, and prevention — aligning with current ACC/AHA 2023 and ESC 2019/2023 guidelines for the management of chronic coronary syndromes and acute coronary syndromes.
Classification of Coronary Artery Disease
CAD is classified based on the acuity of clinical presentation and underlying pathophysiological mechanism, with modern guidelines differentiating chronic coronary syndromes (CCS) from acute coronary syndromes (ACS):
| Classification | Clinical Entity | Pathophysiology | Key Feature |
|---|---|---|---|
| Chronic Coronary Syndromes (CCS) | Stable angina pectoris | Fixed atherosclerotic stenosis (>70% lumen diameter reduction); supply-demand mismatch on exertion | Predictable, reproducible chest pain on exertion; relieved by rest or GTN within 5 min |
| Silent (asymptomatic) ischemia | Coronary stenosis producing objective ischemia without anginal symptoms | Detected by stress testing or imaging; common in diabetics | |
| Ischemic cardiomyopathy | Chronic hypoperfusion and recurrent MI causing LV dysfunction and HFrEF | Dilated cardiomyopathy phenotype from CAD; revascularization may recover "hibernating" myocardium | |
| Coronary artery spasm (Prinzmetal/variant angina) | Focal epicardial coronary vasospasm causing transient total occlusion without significant fixed stenosis | Angina at rest; ST elevation during episode; responds to CCBs and nitrates | |
| Acute Coronary Syndrome (ACS) | Unstable angina (UA) | Plaque rupture / erosion → thrombus → significant but incomplete, transient occlusion; no myocardial necrosis | New-onset angina, rest angina, or crescendo angina; no biomarker elevation; ECG may show ST depression or T-wave inversion |
| NSTEMI | Plaque rupture → subtotal or transient total occlusion → subendocardial myocardial necrosis | Elevated troponin; no persistent ST elevation; ST depression or T-wave changes on ECG | |
| STEMI | Complete occlusion of epicardial coronary artery → transmural myocardial infarction | Persistent ST elevation ≥1 mm (≥2 mm in V1–V3) in ≥2 contiguous leads; elevated troponin; immediate PCI required | |
| Special Forms | MINOCA (MI with non-obstructive coronary arteries) | Plaque disruption, coronary spasm, spontaneous coronary artery dissection (SCAD), or microvascular dysfunction — no obstructive CAD on angiography | More common in younger women; requires specialized investigation (OCT, CMR, provocative testing) |
Signs and Symptoms of Coronary Artery Disease
The clinical presentation of CAD is extraordinarily diverse — from completely asymptomatic (silent ischemia) to catastrophic sudden cardiac death — depending on the degree of coronary stenosis, rate of plaque progression, presence of collateral circulation, individual pain perception thresholds, and whether the presentation is chronic or acute.
Classic Anginal Triad (Meets ALL three criteria):
Substernal chest discomfort with characteristic quality and duration · (2) Provoked by exertion or emotional stress · (3) Relieved by rest and/or sublingual nitroglycerine within 5 minutes. Typical angina = all 3. Atypical angina = 2 of 3. Non-cardiac chest pain = 0–1 of 3.
1. Chest Pain and Angina Pectoris
- Substernal chest pain / pressure — the hallmark of angina: Classic angina is experienced as a deep, heavy pressure, tightness, squeezing, or crushing sensation in the central or left-sided chest — described by patients as "an elephant sitting on the chest," "a band tightening around the chest," or "a vice-like grip." The discomfort typically occupies a diffuse substernal zone rather than a localized, finger-pointed spot (pointing a single finger at the pain site — the "Levine sign" — suggests a cardiac origin). It is characteristically induced by exertion (walking uphill, climbing stairs, sexual activity) or emotional stress and relieved promptly (within 5 minutes) by rest or sublingual glyceryl trinitrate (GTN), which reduces preload and myocardial oxygen demand through venous dilation and reduces afterload through arterial dilation.
- Radiation of chest pain — classical patterns: Anginal discomfort frequently radiates beyond the chest through referred pain pathways sharing common afferent spinal cord segments (T1–T5). The most clinically significant radiation patterns include: left shoulder and medial aspect of the left arm (most classic — ulnar surface of the left forearm and fingers), bilateral arm radiation, jaw, mandible and teeth (mistaken for dental pain), back and interscapular region (particularly in aortic dissection and inferior MI), epigastrium (inferior MI may present with "indigestion" or upper abdominal pain — high-risk misdiagnosis scenario), and neck and throat. Right-sided chest or arm radiation may occur with right coronary artery (RCA) territory ischemia.
- Unstable angina patterns — crescendo angina: A change in the pattern of previously stable angina is a cardiovascular emergency: new-onset angina at rest, nocturnal angina (awakening from sleep), angina occurring at progressively lower exertion thresholds (crescendo pattern), or angina lasting >20 minutes without complete relief from GTN — all represent unstable angina until proven otherwise. These features indicate plaque instability, and patients must be triaged and evaluated urgently for ACS.
- Atypical presentations — particularly in women, elderly, and diabetics: A critical subset of patients — disproportionately including women, elderly individuals (>75 years), diabetic patients (autonomic neuropathy blunts pain perception), and patients with prior cardiac transplantation — present with atypical or absent anginal symptoms despite significant coronary ischemia. Atypical presentations include: burning epigastric discomfort (mimicking GERD or peptic ulcer), isolated dyspnea (the most common "anginal equivalent"), profound unexplained fatigue, nausea and vomiting, jaw or back discomfort without chest pain, diaphoresis without pain, or simple malaise and impending doom. Missing these atypical presentations leads to delayed diagnosis, delayed reperfusion, and worse outcomes — particularly in women who are significantly more likely to present atypically and be misdiagnosed initially.
- Acute myocardial infarction pain: In STEMI, pain is typically severe, sustained (>30 minutes), unrelieved by GTN, and associated with diaphoresis, nausea, vomiting, dyspnea, and a sense of impending doom. The pain of MI is the same in character to angina but far more intense and persistent. Approximately 20–30% of MIs — particularly inferior MIs in diabetics and the elderly — may present with minimal or no chest pain ("silent MI"), detectable only retrospectively on ECG (Q waves, LBBB) or echocardiography (regional wall motion abnormality).
2. Dyspnea and Cardiopulmonary Symptoms
- Exertional dyspnea — the most common anginal equivalent: Breathlessness on exertion that occurs in the absence of or alongside chest discomfort may be the predominant symptom of myocardial ischemia, reflecting transient exercise-induced left ventricular diastolic dysfunction with elevated left atrial pressure causing pulmonary venous congestion. This "dyspnea equivalent" of angina is particularly prevalent in women, elderly patients, and those with diastolic dysfunction — and may be erroneously attributed to pulmonary pathology, deconditioning, or obesity, leading to under-investigation for CAD.
- Orthopnea and paroxysmal nocturnal dyspnea (PND): In established ischemic cardiomyopathy with reduced left ventricular ejection fraction (HFrEF), fluid redistribution on lying flat increases central blood volume and pulmonary venous pressure, causing orthopnea (dyspnea on lying flat, relieved by sitting up — classically graded by the number of pillows required) and PND (abrupt awakening 1–3 hours after sleep onset with severe breathlessness, requiring the patient to sit upright or move to a window for air).
- Acute pulmonary edema: In large STEMI or acute decompensation of ischemic heart failure, sudden severe dyspnea, pink frothy sputum, severe hypoxemia, bilateral crackles, and diaphoresis herald acute cardiogenic pulmonary edema — a medical emergency requiring immediate respiratory and hemodynamic support alongside myocardial reperfusion.
- Palpitations: Ischemia-induced electrical instability of the myocardium generates ventricular ectopic beats, ventricular tachycardia (VT), and ventricular fibrillation (VF). Patients may experience palpitations (awareness of irregular or rapid heartbeat) as a presenting feature of ischemia-provoked arrhythmia — particularly relevant when palpitations are exercise-associated, suggesting ischemia-triggered ventricular ectopy.
3. Neurological and Systemic Symptoms
- Syncope and presyncope: Transient loss of consciousness may accompany severe myocardial ischemia through several mechanisms: (1) cardiogenic syncope from severe reduction in cardiac output during ischemic left ventricular dysfunction; (2) vasovagal reflex syncope triggered by inferior MI (Bezold-Jarisch reflex — vagal activation from inferior wall ischemia causing bradycardia and hypotension); (3) arrhythmic syncope from ischemia-induced VT or VF; and (4) second- or third-degree AV block complicating inferior MI (RCA ischemia interrupts AV nodal blood supply). Any syncope during or after exertion demands urgent cardiac evaluation for CAD and arrhythmias.
- Diaphoresis (profuse sweating): Intense sympathetic activation accompanying myocardial ischemia or infarction produces cold, clammy diaphoresis — a critically important clinical sign that accompanies ACS and cardiogenic shock, and should always prompt urgent evaluation when it coexists with chest discomfort. In contrast to fever-associated sweating, cardiac diaphoresis is characteristically cold and clammy.
- Nausea and vomiting: Vagal stimulation from inferior and inferoposterior MI (supplied by the RCA, whose vagal innervation is particularly dense) causes nausea, vomiting, and bradycardia — the Bezold-Jarisch reflex. These symptoms are frequently misattributed to gastrointestinal pathology, delaying recognition of inferior MI. Vomiting during MI also predisposes to aspiration and electrolyte disturbances.
- Fatigue and exercise intolerance: Chronic fatigue — disproportionate to the level of physical activity — reflects reduced cardiac output from LV systolic or diastolic dysfunction, anemia (which aggravates angina), and the deconditioning accompanying chronic ischemic heart disease. Patients with ischemic cardiomyopathy frequently report profound fatigue that significantly impairs quality of life and daily functioning.
- Anxiety and sense of impending doom: During acute MI, patients frequently report an overwhelming, visceral sense of impending doom or death — a symptom with high specificity for ACS and attributed to massive sympathetic activation, pain intensity, and possibly direct neurological effects of myocardial hypoxia on central nervous system stress pathways. This symptom should never be dismissed as anxiety or panic disorder without appropriate cardiac evaluation.
- Peripheral edema: Bilateral pitting edema of the lower limbs, sacrum (in bedridden patients), and eventually anasarca reflects fluid retention from right ventricular failure secondary to chronic left-sided heart failure from ischemic cardiomyopathy, or right ventricular infarction (a specific complication of inferior STEMI from RCA occlusion). Peripheral edema indicates advanced ischemic heart disease with significant hemodynamic compromise.
4. Physical Examination Findings
- Normal examination in stable CAD: The physical examination is frequently entirely normal in patients with chronic stable angina, as resting coronary flow may be adequate at rest even with significant stenoses — symptoms only arise during exertion when demand exceeds supply. Normal examination does not exclude significant CAD.
- Cardiovascular examination findings: S4 gallop (atrial gallop) — a low-frequency sound best heard at the cardiac apex in early diastole with the bell of the stethoscope, reflecting reduced left ventricular compliance from myocardial ischemia or hypertrophy; S3 gallop — in established heart failure with volume overload; new or changing mitral regurgitation murmur (holosystolic at apex, radiating to axilla) — a critical sign suggesting ischemic papillary muscle dysfunction or rupture complicating acute MI; pericardial friction rub (2–3 component scratching sound) — in pericarditis complicating transmural MI (Dressler's syndrome or early post-infarct pericarditis).
- Signs of heart failure in ischemic cardiomyopathy: Elevated jugular venous pressure (JVP); bilateral basal pulmonary crackles (fine, inspiratory, non-clearing — alveolar edema); displaced apex beat (left and inferolateral displacement beyond the midclavicular line — reflecting LV enlargement); hepatomegaly with pulsatility (in right heart failure); peripheral pitting edema.
- Peripheral vascular examination: Diminished peripheral pulses, carotid bruits (cerebrovascular atherosclerosis), femoral bruits, and absent pedal pulses indicating peripheral arterial disease — a powerful marker of systemic atherosclerosis and high CAD risk. Examination of fundus may reveal hypertensive or diabetic retinopathy — risk factor stigmata.
- Xanthelasma and xanthomata: Periorbital yellowish lipid deposits (xanthelasma) and tendon or eruptive skin xanthomata indicating familial hypercholesterolaemia — a genetic cause of premature and severe CAD.
- Signs of cardiogenic shock in large MI: Hypotension (SBP <90 mmHg for >30 min), cold clammy peripheries, tachycardia, oliguria (<30 mL/hr), and altered consciousness — defining features of cardiogenic shock requiring emergency mechanical support and revascularization.
CAD risk factors have been systematically identified and quantified through decades of longitudinal epidemiological research — most notably the Framingham Heart Study, INTERHEART Study, and SCORE2 Project. The INTERHEART study demonstrated that nine modifiable risk factors account for over 90% of the attributable risk of first MI globally — underscoring the extraordinary preventability of CAD.
1. Non-Modifiable Risk Factors
- Age: Atherosclerosis is a lifelong progressive disease that begins with fatty streak formation in the first decade of life. Clinically significant CAD becomes increasingly prevalent with advancing age as decades of plaque accumulation, oxidative stress, endothelial senescence, and cumulative risk factor exposure lead to hemodynamically significant coronary stenosis and plaque instability. CAD risk accelerates: men face substantial CAD risk from approximately age 45, women from approximately age 55 (post-menopausal). Octogenarians and nonagenarians have near-universal coronary atherosclerosis on post-mortem examination.
- Male sex and hormonal factors: Males develop clinically significant CAD approximately 10 years earlier than females, with substantially higher age-adjusted CAD event rates throughout adulthood. Endogenous estrogen in premenopausal women provides cardioprotective effects through multiple mechanisms — upregulating endothelial nitric oxide synthase (eNOS) promoting vasodilation, improving lipoprotein profiles (elevating HDL, reducing LDL oxidation), attenuating inflammatory responses, and inhibiting smooth muscle cell proliferation. After menopause, the loss of these protective effects narrows the gender gap in CAD risk. Importantly, females with CAD have distinct presentations, less typical anginal symptoms, higher prevalence of MINOCA, and historically poorer evidence-based care, contributing to their worse post-MI outcomes in some studies.
- Family history of premature CAD: A first-degree relative (parent or sibling) with CAD before age 55 (males) or 65 (females) substantially amplifies individual CAD risk — approximately 1.5 to 2-fold over baseline — independent of shared lifestyle factors. This familial risk reflects heritable contributions to atherosclerosis susceptibility through polygenic variation in lipid metabolism, blood pressure regulation, coagulation, inflammation, and endothelial function pathways. Strong family history is a major component of all cardiovascular risk prediction tools and may warrant earlier and more aggressive risk factor screening and pharmacotherapy.
- Familial hypercholesterolaemia (FH) and genetic lipid disorders: FH — caused by autosomal dominant mutations in LDLR (LDL receptor), APOB (apolipoprotein B), or PCSK9 — produces severely elevated LDL-C from birth (LDL-C typically 5–10 mmol/L in heterozygous FH). Without treatment, untreated heterozygous FH causes first MI before age 50 in 50% of males and before age 60 in 30% of females. Homozygous FH (LDL-C >13 mmol/L) causes MI in childhood and adolescence. Lipoprotein(a) — Lp(a) — a genetically determined, largely non-modifiable LDL-like particle carrying additional prothrombotic components — is an independent CAD risk factor elevated in approximately 20% of the population; Lp(a) >50 mg/dL significantly amplifies CAD risk, particularly for premature atherosclerosis.
- Race and ethnicity: South Asian individuals (from the Indian subcontinent, Pakistan, Bangladesh, Sri Lanka) have disproportionately high CAD incidence and mortality — approximately 1.5–2-fold higher than European Caucasians — with earlier onset, more severe angiographic disease, and higher CAD event rates despite lower classical risk factor burden. This disparity reflects greater insulin resistance, higher central adiposity, elevated Lp(a), and specific genetic susceptibility variants in South Asian populations. East Asians generally have lower CAD rates but higher stroke rates compared to European populations. African Americans have higher rates of hypertension-related CAD with distinct risk factor profiles.
2. Major Modifiable Risk Factors
- Dyslipidaemia — elevated LDL cholesterol: The causal role of elevated LDL-C in atherosclerosis and CAD is among the most robustly established relationships in medicine, supported by Mendelian randomization studies, GWAS analyses, statin trials, and the natural experiment of FH. LDL-C enters the arterial intima at concentrations proportional to plasma LDL levels, where it is retained, oxidized, and triggers the inflammatory cascade of atherogenesis. The magnitude of CAD risk reduction is directly proportional to the absolute LDL-C reduction achieved — every 1 mmol/L (38.6 mg/dL) reduction in LDL-C reduces major cardiovascular events by approximately 22% (meta-analysis of statin trials, Lancet). Low HDL-C (<1.0 mmol/L in men, <1.2 mmol/L in women) and elevated triglycerides (>1.7 mmol/L) independently increase CAD risk through impaired reverse cholesterol transport and VLDL-related mechanisms.
- Hypertension (systemic arterial hypertension): Elevated systolic blood pressure — even within the "prehypertension" range (SBP 120–139 mmHg) — accelerates atherosclerosis through endothelial shear stress injury, increased intimal permeability to LDL, oxidative stress activation, RAAS-driven vascular remodeling, and left ventricular hypertrophy that increases myocardial oxygen demand. The relationship between blood pressure and cardiovascular risk is continuous, consistent, and independent — with each 20 mmHg increase in SBP (or 10 mmHg in DBP) associated with a 2-fold increase in cardiovascular mortality. Hypertension is the single most prevalent modifiable CAD risk factor globally, affecting approximately 1.28 billion adults worldwide.
- Diabetes mellitus (Type 1 and Type 2): Diabetes dramatically amplifies CAD risk — conferring a 2–4-fold increase in cardiovascular event risk. Adults with diabetes have CAD equivalent to non-diabetic individuals who have already had a myocardial infarction — explaining why diabetes has historically been classified as a "CAD equivalent" requiring aggressive primary prevention. Mechanisms include advanced glycation end-products (AGEs) accelerating vascular aging, oxidative stress amplifying atherogenesis, insulin resistance driving dyslipidemia (hypertriglyceridemia, low HDL-C, small dense LDL), endothelial dysfunction, platelet hyperreactivity, and impaired fibrinolysis. Diabetic patients with CAD more frequently have diffuse multivessel disease, poor collateral development, higher rates of "silent" ischemia, and worse post-MI outcomes.
- Tobacco smoking: The INTERHEART study identified smoking as responsible for approximately 36% of the population-attributable risk of first MI globally — making it the single largest modifiable CAD risk factor. Tobacco smoke constituents (carbon monoxide, nicotine, polycyclic aromatic hydrocarbons, acrolein, benzene, and oxidant gases) exert multiple cardiovascular effects: endothelial dysfunction through oxidative nitric oxide scavenging, accelerated atherosclerosis through LDL oxidation and foam cell formation, platelet aggregation enhancement, vasospasm, carbon monoxide-mediated reduced oxygen-carrying capacity, and procoagulant state. Heavy smokers (>20 cigarettes/day) have a 3-fold elevated MI risk vs non-smokers. Critically, CAD risk declines significantly within weeks to months after cessation and approaches non-smoker levels within 3–5 years, providing a powerful incentive for cessation at any age.
- Obesity and overweight (central adiposity): Excess body weight — particularly central/visceral adiposity (waist circumference >94 cm in men, >80 cm in women by IDF criteria) — amplifies CAD risk through multiple mechanisms: hypertension, dyslipidemia, insulin resistance and type 2 diabetes, low-grade chronic inflammation from adipokine dysregulation (elevated TNF-α, IL-6, leptin; reduced adiponectin), obstructive sleep apnea, and direct ectopic lipid deposition in cardiac and vascular tissues. Obesity-associated cardiometabolic risk is strongest for central/visceral obesity (reflected by waist-to-hip ratio and waist circumference) more than overall BMI — highlighting the importance of body composition assessment beyond simple BMI measurement.
3. Lifestyle and Behavioral Risk Factors
- Physical inactivity and sedentary behavior: Regular physical activity reduces CAD risk through multiple beneficial effects: lowers blood pressure, improves lipid profile (raises HDL-C, lowers triglycerides), improves insulin sensitivity and glycemic control, reduces body weight and adiposity, reduces inflammatory markers (CRP, IL-6), improves endothelial function through shear stress-mediated eNOS upregulation, promotes coronary collateral development, and reduces sympathetic nervous system tone. Physical inactivity — affecting approximately 27% of the global adult population — is estimated to contribute to approximately 10% of premature deaths. Even modest increases in activity (30 minutes of brisk walking 5 days per week) produce significant cardiovascular risk reduction.
- Unhealthy dietary patterns: Diets high in saturated fats (raising LDL-C), trans-fats (raising LDL-C and lowering HDL-C — the most atherogenic dietary fats), refined carbohydrates and added sugars (driving hypertriglyceridemia and insulin resistance), sodium (hypertension), and processed meats (nitrates, heme iron promoting oxidative stress) substantially elevate CAD risk. The PREDIMED trial demonstrated that a Mediterranean diet supplemented with extra-virgin olive oil or nuts reduced major cardiovascular events by approximately 30% compared to a reduced-fat diet — establishing dietary pattern as a powerful, modifiable cardiovascular risk determinant.
- Psychosocial stress, depression, and mental health: Psychosocial factors — including chronic work stress, social isolation, depression, anxiety, and post-traumatic stress disorder (PTSD) — independently increase CAD risk and worsen prognosis after MI. Depression — present in approximately 20% of MI survivors — triples post-MI mortality risk independently of other risk factors. Mechanisms include HPA axis activation with chronic cortisol elevation promoting atherogenesis, sympathetic nervous system overdrive increasing heart rate and blood pressure, platelet hyperreactivity, inflammatory activation, unhealthy lifestyle behaviors (smoking, inactivity, poor diet), and reduced medication adherence. Screening for depression and psychosocial risk factors is now a component of comprehensive cardiovascular risk assessment in major guidelines.
- Obstructive sleep apnea (OSA): OSA — affecting approximately 30% of adults with hypertension or obesity — is independently associated with CAD risk through repetitive nocturnal hypoxia producing sympathetic activation, oxidative stress, endothelial dysfunction, inflammatory cytokine release, cardiac arrhythmias, and pulmonary hypertension. CPAP therapy effectively treats OSA symptoms and reduces blood pressure but has not definitively demonstrated reduction in cardiovascular events in randomized trials (SAVE, RICCADSA), possibly due to poor CPAP adherence in included trials.
- Excessive alcohol consumption: Heavy chronic alcohol use (>3–4 drinks/day) is a significant cardiovascular risk factor — raising blood pressure, promoting arrhythmias (particularly atrial fibrillation — "holiday heart"), inducing dilated cardiomyopathy (alcoholic cardiomyopathy), and contributing to obesity and dyslipidemia. The previously cited "J-curve" benefit of moderate alcohol — suggesting cardiovascular protection from 1–2 drinks/day — is now substantially questioned by Mendelian randomization studies demonstrating no safe level of alcohol consumption for cardiovascular health.
4. Emerging and Novel Risk Factors
- High-sensitivity C-reactive protein (hsCRP) and systemic inflammation: Atherosclerosis is fundamentally an inflammatory disease, and elevated hsCRP — a sensitive marker of systemic vascular inflammation — independently predicts cardiovascular events beyond classical risk factors. The JUPITER trial demonstrated that rosuvastatin significantly reduced cardiovascular events in individuals with normal LDL-C but elevated hsCRP (>2.0 mg/L), establishing the concept of "residual inflammatory risk" that persists even with optimal LDL-C reduction. The CANTOS trial demonstrated that canakinumab (anti-IL-1β antibody) reduced recurrent MI independent of lipid effects, confirming inflammation as a therapeutic target in CAD.
- Lipoprotein(a) — Lp(a): Lp(a) is a genetically determined LDL-like particle with an additional apolipoprotein(a) component that confers prothrombotic and proinflammatory properties. Elevated Lp(a) (>50 mg/dL or >125 nmol/L) is present in approximately 20–25% of individuals and independently doubles CAD risk. Lp(a) is largely resistant to conventional lipid-lowering therapy; emerging Lp(a)-specific therapies (pelacarsen — antisense oligonucleotide, olpasiran — siRNA) are in Phase III trials targeting Lp(a) reduction for cardiovascular risk reduction.
- Clonal hematopoiesis of indeterminate potential (CHIP): Somatic mutations in hematopoietic stem cells — particularly in DNMT3A, TET2, ASXL1, and JAK2 — that confer a clonal growth advantage emerge naturally with aging (prevalence >10% in those over 70). CHIP-associated clonal leukocytes produce excessive pro-inflammatory cytokines (IL-1β, IL-6, TNF-α) that significantly accelerate atherosclerosis and increase CAD risk by approximately 40–50% — an entirely novel, non-traditional cardiovascular risk mechanism with emerging therapeutic implications (IL-1β inhibition with colchicine or canakinumab).
- Air pollution and environmental exposures: Chronic exposure to fine particulate matter (PM2.5) — from vehicle emissions, industrial pollution, and biomass burning — is associated with a measurable increase in cardiovascular mortality and MI risk. WHO estimates that ambient air pollution causes approximately 4.2 million deaths annually, with a substantial proportion attributable to cardiovascular disease. PM2.5 induces systemic oxidative stress, endothelial dysfunction, platelet activation, and autonomic nervous system dysregulation through pulmonary and direct vascular effects.
Diagnosis of Coronary Artery Disease
Diagnosis of CAD integrates clinical assessment, resting and dynamic electrocardiography, cardiac biomarkers, non-invasive imaging modalities, and invasive coronary angiography. The diagnostic strategy is guided by the clinical presentation: stable CCS allows deliberate stepwise evaluation; ACS demands urgent parallel workup and therapeutic action within defined time windows.
1. Clinical History and Physical Examination
- Symptom characterisation: Onset, duration, character (pressure, tightening, burning), radiation pattern, provoking and relieving factors, severity (CCSS angina classification I–IV for stable angina), and associated symptoms (dyspnea, diaphoresis, nausea, syncope, palpitations). CCSS Class I — angina only with strenuous activity; Class II — slight limitation with vigorous ordinary activity; Class III — marked limitation with mild activity; Class IV — angina at rest or any physical activity.
- Pre-test probability (PTP) assessment: Risk stratification using the ESC 2019 clinical pre-test probability model (based on age, sex, and angina typicality) determines the likelihood of obstructive CAD before testing: <5% PTP — tests unlikely to be beneficial; 5–15% PTP — non-invasive functional testing preferred; 15–85% PTP — coronary CT angiography or functional imaging; >85% PTP — treat empirically or proceed directly to invasive assessment.
- TIMI Risk Score (ACS): For NSTEMI/UA: 7-item score incorporating age ≥65, ≥3 CAD risk factors, prior coronary stenosis ≥50%, ST deviation on ECG, ≥2 anginal events in 24h, aspirin use within 7 days, elevated cardiac markers — score 0–2: low risk; 3–4: intermediate; 5–7: high risk — guides urgency of invasive assessment.
- GRACE Risk Score: Validated in-hospital and 6-month mortality prediction tool for ACS incorporating age, heart rate, systolic BP, serum creatinine, Killip class, cardiac arrest at admission, ST deviation, and elevated cardiac biomarkers — superior discriminatory accuracy to TIMI for risk stratification in NSTEMI.
2. Electrocardiography (ECG)
- Resting 12-lead ECG: The initial, most widely available, and most time-critical diagnostic tool. In stable CAD, the resting ECG is normal in approximately 50% of patients. Relevant findings include: Q waves (≥1 mm wide and ≥2 mm deep — markers of prior full-thickness infarction; location indicates culprit territory), ST depression (subendocardial ischemia or posterior MI), T-wave inversion (ischemia or prior MI), LBBB (new LBBB is a STEMI equivalent requiring immediate reperfusion). In ACS: ST elevation ≥1 mm in ≥2 contiguous limb leads or ≥2 mm in ≥2 contiguous precordial leads in STEMI; reciprocal ST depression in leads remote from the infarct zone (highly specific for transmural MI).
- ECG criteria for specific MI territories: Anterior STEMI (V1–V4) — LAD occlusion; Inferior STEMI (II, III, aVF) — RCA or LCx occlusion; Lateral STEMI (I, aVL, V5–V6) — LCx or diagonal branch; Posterior MI (tall R in V1–V2, ST depression V1–V3) — RCA or LCx; Right ventricular MI (ST elevation in V3R–V4R) — proximal RCA — requires IV fluids not nitrates; Wellens syndrome (deep symmetric T-wave inversions in V2–V3) — critical proximal LAD stenosis, pre-infarction pattern requiring urgent angiography.
- Exercise stress ECG (EST): Standard Bruce protocol treadmill exercise test: ≥1 mm horizontal or downsloping ST depression at peak exercise is the criterion for a positive test. Sensitivity approximately 68%, specificity approximately 77% for obstructive CAD. Particularly valuable in intermediate-PTP patients with interpretable ECG and ability to exercise. Additional prognostic markers: exercise capacity, heart rate response (chronotropic incompetence), angina reproduction, blood pressure response, and recovery ST changes.
- Ambulatory 24-hour Holter ECG: For detection of silent ischemic ST changes, episodic ST depression correlating with symptoms, Prinzmetal's vasospastic angina (ST elevation at rest), and ischemia-triggered arrhythmias. Useful when symptoms are episodic and unpredictably occurring outside structured exercise testing.
3. Cardiac Biomarkers
- High-sensitivity cardiac troponin I and T (hs-cTnI, hs-cTnT): The cornerstone biomarkers for MI diagnosis and ACS risk stratification. Cardiac troponins are structural proteins of the cardiomyocyte contractile apparatus (troponin I and T are cardiac-specific isoforms). Released into the bloodstream within 1–3 hours of myocardial necrosis, troponins rise progressively, peak at 12–24 hours, and remain elevated for 7–14 days (troponin T) or 5–7 days (troponin I). The 0h/1h or 0h/2h high-sensitivity troponin protocols (ESC Rapid Rule-Out) enable rapid MI exclusion: troponin below limit of detection at 0h with low clinical PTP achieves 99.5% negative predictive value for MI, enabling early safe discharge from the emergency department. Troponin elevation must be interpreted in clinical context — non-ACS causes include pulmonary embolism, myocarditis, Takotsubo cardiomyopathy, severe sepsis, renal failure, and heart failure.
- CK-MB (creatine kinase-MB isoenzyme): Less sensitive and cardiac-specific than troponins; rises within 3–6 hours, peaks at 12–24 hours, returns to normal within 48–72 hours — useful for detecting myocardial re-infarction during the same hospitalization (when elevated troponin makes reinfarction detection by troponin alone difficult). CK-MB ratio (CK-MB/total CK >2.5%) improves specificity for myocardial source.
- BNP / NT-proBNP: Natriuretic peptides reflect elevated LV filling pressure and wall stress — elevated in ACS with significant LV dysfunction, acute heart failure, and ischemic cardiomyopathy. NT-proBNP >900 pg/mL in ACS patients is associated with significantly elevated 30-day mortality and aids in risk stratification beyond troponin.
- Lipid profile (total cholesterol, LDL-C, HDL-C, triglycerides, non-HDL-C): Essential for risk stratification and treatment targets. In ACS, lipids measured within 24 hours of MI onset provide the most accurate fasting baseline, as LDL-C falls progressively in the days following MI. High-intensity statin therapy must not be delayed pending lipid results in ACS — initiate immediately and adjust target-based therapy at follow-up.
- HbA1c, fasting glucose, and renal function: Screening for diabetes and CKD — both CAD risk amplifiers. eGFR also essential for contrast media dose calculation in angiography and DOAC dosing if anticoagulation is required.
4. Non-Invasive Cardiac Imaging
A. Echocardiography (TTE)
- Resting TTE: Mandatory in ACS for assessment of global and regional LV systolic function (LVEF), identification of regional wall motion abnormalities (RWMAs) corresponding to ischemic territories, valvular function (new MR in papillary muscle ischemia), pericardial effusion, mechanical complications (VSD, free wall rupture, papillary muscle rupture), and RV function in inferior MI with RV involvement.
- Stress echocardiography: Combines exercise or pharmacological stress (dobutamine infusion for patients unable to exercise) with real-time echocardiographic imaging to detect inducible RWMAs — indicating stress-provoked ischemia in viable myocardium. Sensitivity approximately 80%, specificity approximately 87% for obstructive CAD. Dobutamine stress echo additionally assesses myocardial viability (hibernating myocardium recovers contractility at low-dose dobutamine — low-dose dobutamine response — then worsens at high dose due to ischemia).
- Speckle-tracking strain echocardiography: Advanced quantitative assessment of myocardial deformation that detects subtle regional dysfunction not visible on conventional 2D echo, enabling earlier and more sensitive ischemia detection and scar characterization.
B. Myocardial Perfusion Imaging (MPI)
- Nuclear cardiology (SPECT / PET MPI): Radionuclide-labeled tracers (Tc-99m sestamibi/tetrofosmin for SPECT; Rubidium-82 or N-13-ammonia for PET) are distributed proportionally to myocardial perfusion during stress and rest. Comparative stress-rest imaging identifies ischemia (perfusion defect on stress that normalizes at rest — reversible defect, indicating viable but ischemic myocardium) from fixed defects (scar — irreversible defect). PET MPI provides quantitative absolute myocardial blood flow measurement, detecting diffuse microvascular disease that SPECT may miss. High sensitivity (~91%) for detecting obstructive CAD, with additional prognostic value from LV volumes and LVEF.
- Coronary CT Angiography (CCTA): The preferred non-invasive imaging modality for anatomical assessment of CAD in intermediate-PTP patients per ESC 2019 CCS guidelines. CCTA provides high-resolution cross-sectional images of coronary artery lumen and wall, characterizing stenosis severity (% diameter stenosis), plaque morphology (calcified, mixed, or non-calcified — vulnerable plaques), and coronary anatomy. Excellent negative predictive value (>99%) for obstructive CAD; sensitivity 91–97%, specificity 80–90%. CT-Fractional Flow Reserve (CT-FFR — HeartFlow FFRCT) adds functional significance assessment to anatomical CCTA findings, determining hemodynamic significance of borderline stenoses without invasive catheterization.
- Coronary artery calcium (CAC) scoring: Non-contrast CT quantifying calcium deposits within coronary arteries — reported as the Agatston score (total coronary calcium burden). CAC is a marker of subclinical atherosclerosis burden. CAC = 0 in an intermediate-risk patient confers very low 10-year MACE risk, allowing downgrading of treatment intensity. CAC >400 identifies very high-risk individuals warranting aggressive treatment regardless of clinical risk score. Particularly valuable for risk reclassification in intermediate-risk patients where the decision to initiate statin therapy or aspirin is uncertain.
C. Cardiac Magnetic Resonance Imaging (CMR)
- Stress CMR perfusion / CMR LGE: CMR with adenosine or regadenoson stress detects inducible perfusion defects (ischemia) with sensitivity ~83%, specificity ~87%. Late gadolinium enhancement (LGE) CMR distinguishes ischemic scar (subendocardial-to-transmural gadolinium enhancement in a coronary territory distribution) from non-ischemic cardiomyopathy (midwall or epicardial pattern). Transmural extent of LGE predicts myocardial viability — <50% transmural LGE predicts functional recovery after revascularization; >50% transmural LGE indicates non-viable scar unlikely to improve with revascularization. CMR is the gold standard for myocardial viability assessment and cardiomyopathy characterization.
5. Invasive Coronary Angiography (ICA) and Physiological Assessment
- Coronary angiography (cardiac catheterization): The reference standard for definitive anatomical characterization of coronary anatomy, stenosis location, severity, and extent (single-vessel, two-vessel, or three-vessel CAD; left main coronary artery disease). Performed via transfemoral or transradial arterial access (radial preferred for lower access site bleeding complications — MATRIX trial), contrast injection into coronary ostia, and multiplane fluoroscopic imaging. Angiography guides revascularization strategy (PCI feasibility, SYNTAX score for CABG vs PCI decision-making) and provides real-time guidance for PCI procedures.
- Fractional flow reserve (FFR) and instantaneous wave-free ratio (iFR): Intracoronary physiological indices that measure the hemodynamic significance of angiographically identified stenoses. FFR is measured by advancing a pressure wire across a stenosis during maximal hyperemia (adenosine); FFR ≤0.80 defines a hemodynamically significant stenosis (the DEFER, FAME, FAME 2 trials established FFR-guided PCI superiority over angiography-guided PCI). iFR (≤0.89) is a resting pressure index that avoids adenosine, validated as non-inferior to FFR (DEFINE-FLAIR, iFR-SWEDEHEART). Physiological assessment is essential for intermediate severity stenoses (40–70% diameter stenosis) where angiographic severity alone is an unreliable predictor of ischemia.
- Intravascular imaging — IVUS and OCT: Intravascular ultrasound (IVUS) and optical coherence tomography (OCT) provide cross-sectional imaging of the coronary vessel wall during catheterization, enabling accurate plaque characterization, identification of plaque rupture/erosion sites in ACS, precise stent sizing and apposition assessment, and optimization of PCI outcomes. OCT is particularly valuable for identifying the mechanism of stent failure (under-expansion, malapposition, restenosis, thrombosis) in complex revascularization scenarios.
Complications of Coronary Artery Disease
Complications of CAD encompass the direct consequences of myocardial ischemia and infarction, the hemodynamic sequelae of ventricular remodeling after MI, rhythm and conduction disturbances, and the adverse effects of antithrombotic and revascularization therapies. Recognition and prompt management of complications is critical to survival and long-term outcomes.
A. Acute Mechanical Complications of MI
These dramatic, often fatal complications result from myocardial necrosis and structural failure of the infarcted ventricular wall. They present with sudden hemodynamic collapse and require immediate surgical or interventional management. Incidence has fallen with timely primary PCI reducing infarct size but remains significant in delayed presentations.
- Ventricular septal defect (VSD): Perforation of the interventricular septum from full-thickness anterior (LAD territory, apical VSD) or inferior (RCA territory, basal posterior VSD) infarction, typically presenting 3–7 days post-MI as sudden onset acute hemodynamic deterioration with a new loud, harsh pansystolic murmur at the left sternal border (the oxygen step-up from right atrium to pulmonary artery confirms the left-to-right shunt on pulmonary artery catheterization). The resulting left-to-right shunt overloads the right ventricle and pulmonary circulation, causing acute right heart failure and cardiogenic shock. Mortality without surgery exceeds 90%. Management requires emergency surgical VSD repair or transcatheter closure after temporary hemodynamic stabilization with IABP or LVAD.
- Papillary muscle rupture and acute severe mitral regurgitation: Complete or partial rupture of the posteromedial papillary muscle (supplied exclusively by the RCA — less collateral blood supply and therefore more vulnerable than the anterolateral papillary muscle which has dual LAD/LCx supply) produces acute severe mitral regurgitation with sudden onset pulmonary edema, hemodynamic collapse, and a new loud holosystolic murmur radiating to the axilla. TOE confirms the diagnosis. Emergency mitral valve repair or replacement is life-saving — medical management alone carries >80% in-hospital mortality.
- Left ventricular free wall rupture: Catastrophic perforation of the necrotic free wall of the LV — typically in the anterior or lateral walls following large LAD territory MI — producing acute cardiac tamponade (Beck's triad: hypotension, muffled heart sounds, elevated JVP) with electromechanical dissociation (pulseless electrical activity — PEA). Occurs predominantly in elderly women with anterior MI and is more common in those presenting late without reperfusion. Immediate pericardiocentesis as a temporizing measure and emergency surgical repair are required. Subacute (partial or contained) rupture may allow surgical intervention in selected patients.
- Left ventricular aneurysm: Scar-related thinning and paradoxical outward expansion of the infarcted LV wall (most common at the LV apex after anterior MI), forming a distinct anatomical aneurysm with dysfunctional dyskinetic wall motion. Complications: mural thrombus formation within the aneurysm (risk of systemic embolism, stroke), ventricular arrhythmias arising from the aneurysm borders, and progressive heart failure from reduced effective LV volume. Detected by echocardiography, LV angiography, or CMR. Managed with anticoagulation for mural thrombus and, in refractory arrhythmia or heart failure, surgical LV aneurysmectomy (Dor procedure).
B. Arrhythmic Complications
- Ventricular fibrillation (VF) and sudden cardiac death (SCD): The most feared complication of acute MI — VF-SCD accounts for approximately 50% of all CAD deaths and frequently occurs before the patient reaches hospital. Ischemia-induced regional heterogeneity of electrical refractoriness creates the substrate for VF — particularly in the first 24–48 hours of STEMI (primary VF — does not independently worsen long-term prognosis post-reperfusion) and as a late complication in patients with severe LV dysfunction (secondary VF — indicates poor prognosis). Community-based early defibrillation programs (public access AEDs), bystander CPR training, and widespread ICD implantation in post-MI patients with LVEF ≤35% are the primary strategies reducing SCD incidence.
- Ventricular tachycardia (VT): Both non-sustained VT (NSVT — <30 seconds, hemodynamically tolerated) and sustained VT (>30 seconds or causing hemodynamic compromise) complicate CAD — arising from re-entry circuits around areas of myocardial scar. Accelerated idioventricular rhythm (AIVR) — a slow wide-complex rhythm at 60–100 bpm occurring in the first hours of STEMI — is a benign reperfusion arrhythmia not requiring treatment. Sustained VT causing hemodynamic instability mandates immediate synchronized DC cardioversion; hemodynamically stable VT may be treated with IV amiodarone.
- Atrial fibrillation (AF) in MI: New AF complicates approximately 6–10% of acute MIs, arising from atrial ischemia, elevated atrial filling pressure from LV dysfunction, and inflammatory pericarditis. AF in MI worsens hemodynamics (loss of atrial kick reduces stroke volume by 10–30%), increases thromboembolic risk, and is associated with increased in-hospital and 1-year mortality. Rate control with metoprolol IV or diltiazem, anticoagulation (DOAC preferred), and cardioversion if hemodynamically unstable are the management priorities.
- Bradyarrhythmias and AV block: Sinus bradycardia and first-degree AV block are common benign findings in inferior MI from vagal activation. Mobitz type I (Wenckebach) second-degree AV block is typically nodal (AV nodal ischemia from RCA), transient, and does not require pacing. Mobitz type II second-degree AV block and complete third-degree (complete) heart block with wide-complex escape rhythm indicate infranodal conduction failure — typically from extensive anterior MI with septal involvement (LAD territory) — and represent an indication for temporary transvenous cardiac pacing and assessment for permanent pacemaker implantation.
C. Heart Failure and Cardiogenic Shock
- Acute left ventricular failure and pulmonary edema: Loss of a critical mass of functional myocardium (>25% LV myocardium in acute MI) produces a sudden reduction in LV systolic function and stroke volume, causing elevated LV filling pressures that are transmitted to the pulmonary capillaries — precipitating hydrostatic pulmonary edema. Clinical features include severe dyspnea, orthopnea, pink frothy sputum, diffuse bilateral crackles, hypoxemia, tachycardia, and a third heart sound (S3). Killip classification quantifies acute heart failure severity in MI: Killip I (no heart failure), II (mild failure, S3), III (pulmonary edema), IV (cardiogenic shock).
- Cardiogenic shock: The most severe hemodynamic manifestation of large MI, defined as sustained hypotension (SBP <90 mmHg) with evidence of tissue hypoperfusion (cold clammy extremities, oliguria <30 mL/hr, altered sensorium) in the absence of hypovolemia or vasodilation. Complicates approximately 5–8% of STEMIs, predominantly from large anterior MI with extensive LAD territory loss (>40% LV myocardium necrosed). Hospital mortality remains high at 40–60% despite optimal therapy. Management: immediate primary PCI for culprit lesion (complete revascularization may not improve outcomes — CULPRIT-SHOCK trial showed staged approach superior); inotropes (norepinephrine preferred over dopamine — SOAP II trial); mechanical circulatory support (IABP — limited benefit in RCTs; Impella CP/5.5 — emerging evidence of benefit in severe shock — DanGer Shock trial).
- Chronic ischemic heart failure (ischemic cardiomyopathy): The most common cause of heart failure with reduced ejection fraction (HFrEF) globally, resulting from cumulative myocardial scar from prior MIs and/or chronic hypoperfusion of viable but hibernating myocardium. Management follows HFrEF guidelines: ACE inhibitors/ARBs/ARNI (sacubitril-valsartan), evidence-based beta-blockers (carvedilol, metoprolol, bisoprolol), MRAs (spironolactone, eplerenone), SGLT2 inhibitors (dapagliflozin, empagliflozin — reduce HF hospitalization and cardiovascular death), cardiac resynchronization therapy (CRT) in selected patients with LBBB and LVEF ≤35%, and ICD for SCD prevention.
D. Thromboembolic Complications
- Left ventricular mural thrombus: Intracardiac thrombus forms in akinetic or dyskinetic regions — particularly the LV apex following anterior MI — in the setting of impaired endocardial blood flow creating turbulence and thrombus deposition on the non-contractile endocardial surface. Detected by echocardiography (echo contrast enhancement improves sensitivity) or CMR. Carries significant systemic embolism risk (5–15%), most seriously to the cerebral circulation causing cardioembolic stroke. Management: anticoagulation with VKA (target INR 2–3) or DOAC (rivaroxaban 15 mg twice daily for 3 months — COMMANDER-HF) for 3–6 months until resolution confirmed by imaging.
- Pulmonary embolism: Prolonged immobility after STEMI, right heart failure with elevated right-sided filling pressures, and the hypercoagulable state of acute MI collectively increase pulmonary embolism risk in hospitalized MI patients. Clinical features include new pleuritic chest pain, hemoptysis, tachycardia, and worsening dyspnea — distinguished from MI recurrence by CT pulmonary angiography.
- Stent thrombosis: Acute (<24h), subacute (1–30 days), late (1–12 months), or very late (>12 months) thrombotic occlusion of a coronary stent — a catastrophic complication presenting as sudden onset STEMI with 45% in-hospital mortality. Caused by dual antiplatelet therapy non-adherence, mechanical stent factors (under-expansion, malapposition, geographic miss), or prothrombotic conditions. Prevention: dual antiplatelet therapy (aspirin + P2Y12 inhibitor — ticagrelor or prasugrel preferred over clopidogrel for 12 months post-ACS); lifelong aspirin; avoidance of elective surgery <3 months post-stenting.
Treatment of Coronary Artery Disease
CAD treatment is stratified by the clinical presentation — chronic coronary syndrome vs acute coronary syndrome — and integrates lifestyle modification, optimal medical therapy (OMT), and coronary revascularization where indicated. All strategies aim to relieve ischemic symptoms, prevent MI and its complications, and reduce cardiovascular mortality.
A. Medical Therapy — The Foundation of CAD Management
1. Antiplatelet Therapy
- Aspirin (75–100 mg daily — lifelong): Irreversibly acetylates COX-1, blocking thromboxane A2-mediated platelet aggregation. The cornerstone of CAD secondary prevention — reduces MI, stroke, and vascular death by approximately 25% in high-risk patients. Loading dose 300 mg for ACS to achieve rapid platelet inhibition before PCI.
- P2Y12 receptor inhibitors — dual antiplatelet therapy (DAPT): Mandatory for 12 months after ACS (aspirin + ticagrelor 90 mg twice daily or prasugrel 10 mg daily — preferred over clopidogrel 75 mg daily based on PLATO and TRITON-TIMI 38 trials demonstrating superior efficacy); DAPT for 1–6 months after elective PCI with drug-eluting stent in stable CAD (duration individualized by ischemic vs bleeding risk — STOPDAPT-2, MASTER-DAPT trials). Ticagrelor and prasugrel provide faster, more consistent platelet inhibition and do not require hepatic bioactivation (unlike clopidogrel, which requires CYP2C19 for conversion to active metabolite — CYP2C19 poor metabolizers have reduced clopidogrel efficacy).
- Cangrelor (IV P2Y12 inhibitor): Rapid-acting, reversible, intravenous P2Y12 inhibitor for bridging antiplatelet therapy during PCI in patients unable to take oral agents; onset within minutes; offset within 1 hour of cessation.
2. Lipid-Lowering Therapy
- High-intensity statin therapy (first-line, all ASCVD patients): Atorvastatin 40–80 mg or rosuvastatin 20–40 mg daily — initiated immediately in all ACS patients regardless of baseline LDL-C. LDL-C target: <1.4 mmol/L (<55 mg/dL) with ≥50% LDL-C reduction from baseline for very-high-risk patients (ESC 2021); <1.0 mmol/L for recurrent ASCVD within 2 years (ESC 2021 extreme-risk target). Statins additionally reduce inflammation (hsCRP) and plaque stabilization (pleiotropic effects) beyond lipid lowering.
- Ezetimibe (10 mg daily): Intestinal cholesterol absorption inhibitor added to maximally tolerated statin if LDL-C target not achieved — provides additional ~15–20% LDL-C reduction. IMPROVE-IT trial demonstrated significant cardiovascular event reduction with ezetimibe added to statin post-ACS (7 years follow-up).
- PCSK9 inhibitors (evolocumab 140 mg Q2W or alirocumab 75–150 mg Q2W — subcutaneous): Monoclonal antibodies inhibiting PCSK9 (which normally degrades LDL receptors on hepatocytes) — dramatically reduce LDL-C by 50–60% on top of statin + ezetimibe. FOURIER (evolocumab) and ODYSSEY OUTCOMES (alirocumab) trials demonstrated significant cardiovascular event reduction in post-MI patients with LDL-C persistently above target despite maximally tolerated statin + ezetimibe. Inclisiran (small interfering RNA targeting PCSK9 mRNA) — twice-yearly subcutaneous injection achieving similar LDL-C reduction — now approved for secondary prevention.
3. Beta-Blockers
Beta-1 selective beta-adrenergic receptor blockers (metoprolol succinate, bisoprolol, carvedilol) reduce myocardial oxygen demand by reducing heart rate, blood pressure, and myocardial contractility — relieving angina, preventing ischemia during physical stress, and reducing arrhythmia risk. Mandatory post-STEMI for all patients with reduced LVEF (HFrEF) — carvedilol, bisoprolol, and metoprolol succinate are the evidence-based agents demonstrating mortality reduction in post-MI HFrEF (CAPRICORN, CIBIS II, MERIT-HF trials). For stable angina, beta-blockers are first-line antianginal therapy in most patients.
4. Renin-Angiotensin-Aldosterone System (RAAS) Blockade
- ACE inhibitors (ramipril, lisinopril, perindopril): Reduce RAAS activation, lower blood pressure, reduce LV afterload, and attenuate post-MI ventricular remodeling. Mandatory in all post-MI patients with LVEF <40%, hypertension, diabetes, or CKD. The HOPE trial demonstrated ramipril reduces cardiovascular events even in patients without LV dysfunction or heart failure — establishing ACE inhibitor use across the high-risk CAD spectrum. Target: maximum tolerated dose.
- ARBs (valsartan, candesartan): Alternative when ACE inhibitors are intolerable (persistent dry cough — bradykinin-mediated). Non-inferior to ACE inhibitors in post-MI heart failure (VALIANT trial).
- ARNI (sacubitril-valsartan, Entresto): Superior to enalapril in reducing cardiovascular death and HF hospitalization in established HFrEF (PARADIGM-HF trial) — now the preferred RAAS agent for symptomatic HFrEF post-MI, replacing ACE inhibitors/ARBs in appropriate candidates.
- Mineralocorticoid receptor antagonists (spironolactone, eplerenone): Eplerenone post-MI with LVEF ≤40% and diabetes or symptomatic heart failure reduces cardiovascular mortality (EPHESUS trial, RRR 15%). Mandatory in post-MI HFrEF alongside ACE inhibitor/ARNI and beta-blocker.
5. SGLT2 Inhibitors — Cardioprotective Class
Sodium-glucose cotransporter-2 inhibitors (dapagliflozin 10 mg daily, empagliflozin 10 mg daily) reduce HF hospitalization and cardiovascular death in patients with established ASCVD or HFrEF regardless of diabetes status (DAPA-HF, EMPEROR-Reduced, EMPA-REG OUTCOME). Mechanisms beyond glycosuria include diuresis, natriuresis, reduced cardiac preload and afterload, anti-inflammatory effects, and myocardial energy substrate optimization. Now a mandatory component of the HFrEF "fantastic four" guideline-directed medical therapy (GDMT) quadruple therapy — ARNI + beta-blocker + MRA + SGLT2i.
6. Antianginal Medications (Symptom Relief in Stable CAD)
- Nitrates (sublingual GTN 0.3–0.6 mg, ISDN, ISMN — long-acting): Venous vasodilation reduces LV preload and myocardial wall tension; coronary vasodilation improves distal coronary flow. Short-acting GTN spray for acute angina relief; long-acting nitrates for prophylaxis. Tolerance (tachyphylaxis) develops with continuous use — nitrate-free interval of 10–12 hours required. Absolutely contraindicated with PDE-5 inhibitors (sildenafil, tadalafil) due to life-threatening hypotension from combined vasodilation.
- Calcium channel blockers (amlodipine, diltiazem, verapamil): Reduce myocardial oxygen demand (negative chronotropy and inotropy — diltiazem/verapamil), promote coronary vasodilation (all CCBs), and reduce peripheral vascular resistance. First-choice antianginals in Prinzmetal's vasospastic angina; complementary to beta-blockers in exertional stable angina. NDHPs (diltiazem, verapamil) contraindicated in HFrEF or with concurrent beta-blockers (risk of bradycardia and AV block).
- Ranolazine (500–1000 mg twice daily): Late sodium channel inhibitor reducing intracellular calcium overload in ischemic myocardium — reduces angina frequency and nitroglycerin consumption without affecting heart rate or blood pressure. Approved as second-line antianginal agent (CARISA trial). Also reduces ventricular arrhythmias in CAD.
- Ivabradine (5–7.5 mg twice daily): Selective If channel inhibitor in the sinoatrial node — reduces heart rate without affecting myocardial contractility. Used for angina and HFrEF (BEAUTIFUL, SHIFT trials) when beta-blockers are contraindicated or maximally tolerated dose insufficient for heart rate control. Target resting HR <60–70 bpm.
B. Coronary Revascularization
7. Percutaneous Coronary Intervention (PCI)
Primary PCI is the preferred reperfusion strategy for STEMI within 12 hours of symptom onset (superiority over thrombolysis demonstrated across all major outcomes in direct comparisons — DANAMI-2, PRAGUE-2, GUSTO IIb). Drug-eluting stents (DES — second-generation thin-strut DES with biocompatible or biodegradable polymer coating — zotarolimus-eluting, everolimus-eluting) are preferred over bare-metal stents due to significantly lower restenosis rates (<5% vs 25%). Techniques:
- Stent implantation: Coronary angioplasty (balloon dilation) followed by DES deployment to scaffold the stenotic segment and maintain luminal patency. OCT/IVUS-guided PCI optimizes stent apposition, expansion, and edge dissection detection — associated with improved outcomes.
- Physiological guidance (FFR/iFR): Mandatory for non-infarct-related artery PCI decisions in multivessel disease ACS — FFR-guided complete revascularization in hemodynamically stable STEMI with multivessel disease reduces MACE versus infarct-only PCI (COMPLETE trial).
- Rotational atherectomy (RA): High-speed diamond-tipped burr ablating heavily calcified lesions that cannot be adequately dilated by conventional balloons — enabling subsequent stent expansion in complex lesion subsets.
- Mechanical circulatory support (Impella, IABP, VA-ECMO): Hemodynamic support during high-risk PCI in cardiogenic shock or severe LV dysfunction.
8. Coronary Artery Bypass Grafting (CABG)
Cardiac surgical revascularization — constructing bypass conduits from the aorta or native vessels to coronary arteries distal to the obstruction — is preferred over PCI in specific anatomical and clinical scenarios proven by landmark trials:
- Left main coronary artery disease: LMCA stenosis ≥50% — CABG preferred for high SYNTAX scores; PCI non-inferior for low-intermediate SYNTAX scores (EXCEL, NOBLE trials). Unprotected LMCA disease with cardiogenic shock or ACS: urgent CABG or PCI depending on anatomy and surgical risk.
- Three-vessel CAD with high SYNTAX score (≥33): Surgical revascularization demonstrated superior survival and lower MACE compared to PCI at 5-year follow-up in the SYNTAX trial. Complete anatomical revascularization is more consistently achieved with CABG than PCI in complex multivessel disease.
- Diabetes mellitus + multivessel CAD: CABG demonstrated significantly superior 5-year survival compared to PCI in diabetics with multivessel disease (FREEDOM trial) — preferential revascularization of multiple territories with LIMA-LAD graft provides superior long-term event-free survival.
- Conduit selection: Left internal mammary artery (LIMA) to LAD graft — the gold standard conduit with >95% patency at 10 years and proven survival benefit (Lytle et al.); bilateral IMA (BIMA) grafting improves long-term outcomes but increases sternal wound complication risk in diabetics; radial artery grafts superior to saphenous vein for non-LAD targets (RADIAL trial); saphenous vein grafts — 50% occlusion rate at 10 years.
9. Emergency Management of STEMI — "Time is Muscle"
- Oxygen: Only if SpO₂ <90% — routine oxygen in normoxic STEMI patients increases infarct size (AVOID trial).
- Aspirin 300 mg oral loading + P2Y12 inhibitor (ticagrelor 180 mg or prasugrel 60 mg) immediately upon STEMI diagnosis.
- Unfractionated heparin (UFH) or bivalirudin: Anticoagulation during PCI to prevent catheter thrombus formation.
- Primary PCI within 90 min (FMC-to-device): Emergency coronary angiography and stenting of the infarct-related artery. GPIIb/IIIa inhibitors (tirofiban, eptifibatide) as bailout therapy for large thrombus burden at PCI.
- Fibrinolysis (thrombolysis): If primary PCI is unavailable within 120 min — alteplase, tenecteplase, or reteplase administered within 12 hours; requires subsequent angiography within 3–24 hours (pharmaco-invasive strategy — STREAM-2 trial).
- Cardiac monitoring, defibrillator availability, and ICU-level care throughout the acute phase.
Prevention of Coronary Artery Disease
CAD prevention operates at three levels: primordial prevention (preventing the development of risk factors in the first place through societal health policies), primary prevention (reducing cardiovascular events in individuals with risk factors but no established CAD), and secondary prevention (preventing recurrent events after established CAD). Prevention is arguably the most powerful intervention in the CAD management arsenal — the majority of MI deaths are preventable.
A. Lifestyle Modification — The Cornerstone of Prevention
- Dietary modification — Mediterranean and DASH dietary patterns: The Mediterranean diet — emphasizing extra-virgin olive oil as the primary fat source, abundant vegetables, fruits, whole grains, legumes, fish, nuts, and red wine in moderation, with limited red meat and processed foods — reduces cardiovascular events by approximately 30% compared to a low-fat diet (PREDIMED trial). The DASH diet (Dietary Approaches to Stop Hypertension) significantly reduces blood pressure and dyslipidemia. Specific dietary recommendations: reduce saturated fat to <7% of total calories; eliminate industrial trans-fats; reduce dietary sodium to <2.3 g/day; increase omega-3 fatty acids (oily fish 2× weekly or supplementation — REDUCE-IT trial: icosapentaenoic acid 4 g/day reduces cardiovascular events in statin-treated hypertriglyceridemic patients); limit added sugars; increase dietary fiber (soluble fiber reduces LDL-C by 5–7%).
- Regular physical activity: Target at minimum 150 minutes per week of moderate-intensity aerobic activity (brisk walking, swimming, cycling) or 75 minutes of vigorous-intensity activity, supplemented by resistance training twice weekly. Regular exercise reduces SBP by 5–8 mmHg, raises HDL-C by 3–6%, reduces triglycerides, improves insulin sensitivity, promotes weight loss, reduces inflammatory markers, and improves cardiac autonomic regulation. Cardiac rehabilitation programs — supervised structured exercise with risk factor management and patient education — reduce all-cause mortality by 26% and cardiovascular mortality by 36% after MI (AHA meta-analysis), representing one of the most powerful secondary prevention interventions available.
- Smoking cessation: The single most impactful lifestyle modification for CAD risk reduction. Cessation reduces CAD risk rapidly and progressively: within 24 hours, platelet reactivity and carbon monoxide levels normalize; within 3 months, pulmonary function and endothelial function improve; within 1 year, excess MI risk decreases by approximately 50%; within 5–15 years, risk approaches that of never-smokers. All patients with CAD or at high CAD risk should receive evidence-based cessation support: brief physician counseling, nicotine replacement therapy (NRT — patches, gum, lozenges), varenicline (most effective pharmacotherapy — 30% 6-month abstinence rate vs 12% for placebo), or bupropion.
- Weight management: Achieving and maintaining a healthy BMI (20–25 kg/m²) and waist circumference through sustainable calorie-appropriate diet and regular exercise. Even modest weight loss (5–10% of body weight) produces clinically meaningful improvements in blood pressure, LDL-C, triglycerides, glycemic control, and inflammatory markers. Weight loss medications (GLP-1 receptor agonists — semaglutide, liraglutide) are increasingly demonstrating cardiovascular benefit: semaglutide 2.4 mg weekly reduced major adverse cardiovascular events by 20% in obese/overweight patients with cardiovascular disease (SELECT trial, 2023).
- Stress management and mental health optimization: Mindfulness-based stress reduction (MBSR), cognitive behavioral therapy (CBT), regular aerobic exercise (potent antidepressant), social connection programs, sleep optimization, and pharmacotherapy for clinical depression (SSRIs are cardiovascularly safe and appropriate first-line agents for post-MI depression — sertraline demonstrated safety in SADHART trial). Screening for depression and anxiety in all CAD patients using validated tools (PHQ-9) and providing evidence-based treatment is a Class I recommendation in ACC/AHA guidelines.
B. Pharmacological Primary Prevention
- Statin therapy for primary prevention: Initiated for individuals with 10-year ASCVD risk ≥7.5–10% (per ACC/AHA Pooled Cohort Equation) who do not achieve targets through lifestyle modification alone; or regardless of risk score in patients with LDL-C >4.9 mmol/L (FH), diabetes age ≥40 years with additional risk factors, or CKD. Multiple large trials (WOSCOPS, AFCAPS/TexCAPS, JUPITER) established statin efficacy for primary prevention. The "ABCDE" approach — Aspirin (not routinely recommended for primary prevention in low-to-intermediate risk due to bleeding risk outweighing benefits — ARRIVE, ASPREE trials), Blood pressure, Cholesterol, Diabetes, Exercise — provides a framework for primary prevention drug therapy decisions.
- Antihypertensive therapy: Treat hypertension to targets <130/80 mmHg with lifestyle modification as foundation; pharmacotherapy with ACE inhibitors/ARBs, thiazide diuretics, or CCBs as initial agents, tailored to comorbidities (ACE inhibitors preferred in diabetes; CCBs for isolated systolic hypertension in elderly; ARBs if ACE inhibitor intolerant).
- Diabetes prevention and management: Intensive lifestyle modification (Mediterranean diet + 150 min/week activity + weight loss ≥5%) reduces T2DM incidence by 58% in individuals with prediabetes (Diabetes Prevention Program). In established T2DM, GLP-1RAs (semaglutide, liraglutide) and SGLT2 inhibitors provide cardiovascular risk reduction beyond glycemic control and should be prioritized in patients with established ASCVD or high cardiovascular risk.
- Colchicine for residual inflammatory risk: Low-dose colchicine 0.5 mg daily — an anti-inflammatory agent targeting NLRP3 inflammasome and microtubule-mediated neutrophil activation — significantly reduces recurrent MACE by 23% in patients with chronic CAD (LoDoCo2 trial) and by 31% following recent MI (COLCOT trial), representing a novel anti-inflammatory strategy targeting residual inflammatory risk beyond optimal statin therapy.
- Aspirin for secondary prevention: Aspirin 75–100 mg daily is a mandatory, indefinite secondary prevention therapy for all patients with established CAD (ACS, stable CAD, post-PCI, post-CABG), where the net benefit unambiguously exceeds bleeding risk.
C. Population-Level and Systemic Prevention
- Cardiovascular risk screening programs: Opportunistic and systematic cardiovascular risk assessment in primary care using validated risk prediction tools (Framingham Risk Score, SCORE2, ACC/AHA Pooled Cohort Equations, JBS3 risk calculator) identifies high-risk individuals who benefit from early preventive intervention before the first clinical event. Coronary artery calcium (CAC) scoring as a supplementary risk-reclassification tool resolves treatment uncertainty in intermediate-risk patients.
- Public health and government policy interventions: Food industry regulation targeting trans-fat elimination from the food supply (Denmark's complete ban on industrial trans-fats reduced cardiovascular disease mortality within years); sodium reduction in processed foods; front-of-pack nutritional labeling; tobacco taxation, plain packaging, and public smoking bans (Ireland's 2004 national smoking ban was associated with significant reductions in acute MI hospitalisations within one year); sugar taxation; urban planning promoting active transport (cycling infrastructure, walkable cities); and air quality regulation limiting PM2.5 levels.
- Cardiac rehabilitation and secondary prevention programs: Comprehensive, structured, evidence-based secondary prevention programs combining supervised exercise training, medication optimization, dietary counseling, smoking cessation support, psychological intervention, and patient education — delivered in group outpatient settings or increasingly via digital/telehealth platforms — reduce recurrent MI by 20%, cardiovascular mortality by 26%, and hospital readmissions by 28% at 3 years. Despite proven benefits, cardiac rehabilitation remains chronically under-utilized, with participation rates of only 25–35% in many high-income countries and far lower in low-to-middle income countries.
- AI and digital health for CAD prevention: Artificial intelligence-powered ECG analysis algorithms detect subclinical CAD, arrhythmias, and LV dysfunction in asymptomatic individuals at scale — enabling population-level cardiovascular screening. Smartwatch-based heart rate and rhythm monitoring, wearable blood pressure monitoring, and remote lipid testing are democratizing cardiovascular risk assessment. AI-driven precision medicine approaches are beginning to enable individualized cardiovascular risk prediction incorporating genomic, proteomic, and imaging biomarkers.
Common FAQs on Coronary Artery Disease
1. What is Coronary Artery Disease (CAD)?
2. What are the early warning signs of CAD?
3. How is CAD diagnosed?
4. What is the difference between angina and a heart attack?
5. What is the best treatment for blocked coronary arteries?
6. Can CAD be reversed or cured?
7. Why do statins play a central role in CAD treatment?
8. What is the Framingham Risk Score?
9. What is STEMI and why is it a medical emergency?
10. What are the lifestyle changes that most effectively prevent CAD?
11. What is the difference between PCI and CABG?
12. How does diabetes increase CAD risk?
13. What is cardiac rehabilitation and who should attend?
14. What is silent myocardial ischemia?
15. What emerging treatments are transforming CAD management?
Bibliography on Coronary Artery Disease
- Knuuti J, Wijns W, Saraste A, et al. 2019 ESC Guidelines for the diagnosis and management of chronic coronary syndromes. European Heart Journal. 2020;41(3):407–477.
- Collet JP, Thiele H, Barbato E, et al. 2020 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation. European Heart Journal. 2021;42(14):1289–1367.
- Ibanez B, James S, Agewall S, et al. 2017 ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation. European Heart Journal. 2018;39(2):119–177.
- Maron DJ, Hochman JS, Reynolds HR, et al. Initial Invasive or Conservative Strategy for Stable Coronary Disease. New England Journal of Medicine. 2020;382(15):1395–1407. [ISCHEMIA Trial]
- Stone GW, Maehara A, Lansky AJ, et al. A Prospective Natural-History Study of Coronary Atherosclerosis. New England Journal of Medicine. 2011;364(3):226–235. [PROSPECT Trial]
- Sabatine MS, Giugliano RP, Keech AC, et al. Evolocumab and Clinical Outcomes in Patients with Cardiovascular Disease. New England Journal of Medicine. 2017;376(18):1713–1722. [FOURIER Trial]
- Lichtenstein AH, Appel LJ, Vadiveloo M, et al. 2021 Dietary Guidance to Improve Cardiovascular Health: A Scientific Statement From the American Heart Association. Circulation. 2021;144(23):e472–e487.
- Estruch R, Ros E, Salas-Salvadó J, et al. Primary Prevention of Cardiovascular Disease with a Mediterranean Diet Supplemented with Extra-Virgin Olive Oil or Nuts. New England Journal of Medicine. 2018;378(25):e34. [PREDIMED Trial Updated]
- Mahaffey KW, Wojdyla DM, Carroll K, et al. Ticagrelor Compared with Clopidogrel by Geographic Region in the Platelet Inhibition and Patient Outcomes (PLATO) Trial. Circulation. 2011;124(5):544–554. [PLATO Trial]
- Nissen SE, Tuzcu EM, Schoenhagen P, et al. Effect of Intensive Compared with Moderate Lipid-Lowering Therapy on Progression of Coronary Atherosclerosis. JAMA. 2004;291(9):1071–1080. [REVERSAL Trial — statin plaque regression]
- Tardif JC, Kouz S, Waters DD, et al. Efficacy and Safety of Low-Dose Colchicine after Myocardial Infarction. New England Journal of Medicine. 2019;381(26):2497–2505. [COLCOT Trial]
- Ryan JJ, Bhatt DL, Bhatt DL, et al. Semaglutide and Cardiovascular Outcomes in Obesity without Diabetes. New England Journal of Medicine. 2023;389(24):2221–2232. [SELECT Trial]
- Farkouh ME, Domanski M, Sleeper LA, et al. Strategies for Multivessel Revascularization in Patients with Diabetes. New England Journal of Medicine. 2012;367(25):2375–2384. [FREEDOM Trial]
- Serruys PW, Morice MC, Kappetein AP, et al. Percutaneous Coronary Intervention versus Coronary-Artery Bypass Grafting for Severe Coronary Artery Disease. New England Journal of Medicine. 2009;360(10):961–972. [SYNTAX Trial]
- Harrison's Principles of Internal Medicine, 21st ed. Editors: Jameson JL, Fauci AS, Kasper DL, Hauser SL, Loscalzo J. McGraw-Hill Education. Chapters: Ischemic Heart Disease; Acute Myocardial Infarction; Heart Failure.