










Acute Respiratory Distress Syndrome (ARDS) – Sign and Symptoms, Risk factors, Diagnosis, Complications, Treatment and Prevention
Acute Respiratory Distress Syndrome (ARDS) is a life-threatening form of diffuse inflammatory lung injury characterized by acute-onset hypoxemic respiratory failure, bilateral pulmonary infiltrates, and reduced lung compliance — not fully explained by cardiac failure or fluid overload. It represents the most severe manifestation of acute lung injury and is among the most challenging conditions managed in the intensive care unit (ICU). ARDS was first formally described by Ashbaugh and colleagues in 1967, who identified a syndrome of acute onset dyspnea, tachypnea, cyanosis refractory to oxygen therapy, diffuse alveolar infiltrates on chest radiography, and decreased lung compliance across 12 patients. Decades of refinement culminated in the Berlin Definition (2012), which replaced the earlier American-European Consensus Conference (AECC) criteria and remains the current diagnostic standard. Acute Respiratory Distress Syndrome (ARDS) is not a single disease but a common clinical syndrome arising from diverse insults — both pulmonary and extrapulmonary — that converge on a shared pathological endpoint: diffuse alveolar damage (DAD), flooding of the alveolar space with protein-rich edematous fluid, and catastrophic impairment of gas exchange. The resulting hypoxemia is characteristically refractory to supplemental oxygen alone. The epidemiology of ARDS is substantial. Estimates suggest an incidence of 10–86 cases per 100,000 person-years, with significant variation by population and ARDS severity. In the United States alone, approximately 190,000 cases occur annually. ICU prevalence data from the LUNG SAFE study (2016), the largest prospective international cohort, found ARDS accounted for 10.4% of all ICU admissions and 23.4% of patients receiving mechanical ventilation across 50 countries. Despite decades of research, overall mortality remains approximately 35–46%, with severe ARDS carrying mortality rates exceeding 45%. ARDS is thus not merely an ICU challenge — it is a global public health emergency.
Acute Respiratory Distress Syndrome (ARDS) is not a single disease but a common clinical syndrome arising from diverse insults — both pulmonary and extrapulmonary — that converge on a shared pathological endpoint: diffuse alveolar damage (DAD), flooding of the alveolar space with protein-rich edematous fluid, and catastrophic impairment of gas exchange. The resulting hypoxemia is characteristically refractory to supplemental oxygen alone. The epidemiology of ARDS is substantial. Estimates suggest an incidence of 10–86 cases per 100,000 person-years, with significant variation by population and ARDS severity. In the United States alone, approximately 190,000 cases occur annually. ICU prevalence data from the LUNG SAFE study (2016), the largest prospective international cohort, found ARDS accounted for 10.4% of all ICU admissions and 23.4% of patients receiving mechanical ventilation across 50 countries. Despite decades of research, overall mortality remains approximately 35–46%, with severe ARDS carrying mortality rates exceeding 45%. ARDS is thus not merely an ICU challenge — it is a global public health emergency.
Pathophysiology of Acute Respiratory Distress Syndrome (ARDS)
Phases of Lung Injury
The pathological evolution of ARDS follows three overlapping phases, though not all patients progress through each stage:
1. Phase 1 — Exudative Phase (Days 0–7)
The exudative phase is the earliest and most clinically acute stage, driven by a cascade of innate immune activation and endothelial–epithelial injury.
The initiating insult — whether direct (e.g., aspiration, pneumonia) or indirect (e.g., sepsis, pancreatitis) — triggers activation of alveolar macrophages, which release pro-inflammatory cytokines including interleukin-1β (IL-1β), IL-6, IL-8, and tumor necrosis factor-alpha (TNF-α). These cytokines recruit and activate neutrophils, which transmigrate across the alveolar-capillary membrane. Activated neutrophils release proteases, reactive oxygen species (ROS), and neutrophil extracellular traps (NETs), inflicting direct cellular injury on both the capillary endothelium and the alveolar epithelium.
The consequences are twofold and simultaneous:
- Endothelial injury disrupts tight junctions of the pulmonary capillary wall, increasing vascular permeability. Protein-rich, edematous fluid floods the interstitium and alveolar spaces — the hallmark of non-cardiogenic pulmonary edema.
- Epithelial injury targets both type I pneumocytes (which constitute 95% of the alveolar surface and are responsible for structural integrity) and type II pneumocytes (responsible for surfactant production and serving as progenitor cells for alveolar repair). Loss of type I cells denudes the basement membrane; loss of type II cells critically impairs surfactant synthesis.
Surfactant depletion and inactivation — driven by dilution by protein-rich edema fluid and direct inactivation by inflammatory mediators — dramatically increases alveolar surface tension. This promotes alveolar collapse (atelectasis), reduces lung compliance, and exacerbates ventilation-perfusion (V/Q) mismatch. The resulting intrapulmonary shunting is the primary mechanism of the severe, refractory hypoxemia that defines ARDS.
Hyaline membranes — composed of plasma proteins, fibrin, and cellular debris — deposit along the alveolar walls, further impairing gas diffusion. On gross pathology, the lungs are heavy, firm, and airless ("hepatized"), reflecting the extent of alveolar flooding and atelectasis.
2. Phase 2 — Proliferative Phase (Days 7–21)
If the patient survives the exudative phase, a repair process begins. Type II pneumocytes proliferate and differentiate into type I cells to restore the alveolar epithelium. Fibroblasts migrate into the alveolar space, and early collagen deposition begins. Simultaneously, the alveolar edema is gradually reabsorbed by restored epithelial sodium-potassium ATPase activity, and surfactant production partially recovers.
Clinically, patients in this phase may begin to show improving oxygenation and weaning from ventilator support. However, some patients fail to resolve inflammation effectively, transitioning instead to the fibrotic phase.
3. Phase 3 — Fibrotic Phase (>21 Days)
A proportion of patients — particularly those with persistent inflammation, prolonged mechanical ventilation, or secondary infections — develop progressive pulmonary fibrosis. Dysregulated fibroblast proliferation and excessive collagen deposition obliterate the alveolar architecture, resulting in honeycombing and cyst formation visible on CT imaging. The fibrotic phase is associated with severe, persistent hypoxemia, markedly reduced lung compliance, increased pulmonary dead space, and substantially elevated mortality.
Mechanical Consequences: The "Baby Lung" Concept
CT imaging of ARDS lungs reveals heterogeneous injury: dependent lung zones are densely consolidated and non-aerated, while non-dependent zones may retain near-normal aeration. The volume of recruitable, aerated lung parenchyma is dramatically reduced — sometimes to the equivalent of a "baby lung" of only 200–400 mL effective volume in a standard adult. This concept, advanced by Gattinoni and colleagues, has profound implications: applying standard tidal volumes (10–12 mL/kg) delivers all ventilation to a small, relatively normal lung region, generating dangerous overdistension (volutrauma) and shear stress (atelectrauma) — the basis of ventilator-induced lung injury (VILI).
Pulmonary Vascular Pathology
Pulmonary hypertension is a near-universal feature of ARDS. It arises from hypoxic vasoconstriction, microthrombi in pulmonary capillaries, and obliteration of the vascular bed by edema and consolidation. Right ventricular (RV) afterload increases markedly, predisposing to acute cor pulmonale — a significant contributor to mortality in severe ARDS. This interaction between the lung and RV must be carefully considered during ventilator management.
Signs and Symptoms of Acute Respiratory Distress Syndrome (ARDS)
ARDS manifests as a clinical syndrome rather than a discrete disease, and its presentation reflects both the underlying precipitating condition and the degree of lung injury. The cardinal clinical features are acute-onset dyspnea, hypoxemia refractory to supplemental oxygen, and diffuse bilateral opacities on chest imaging. 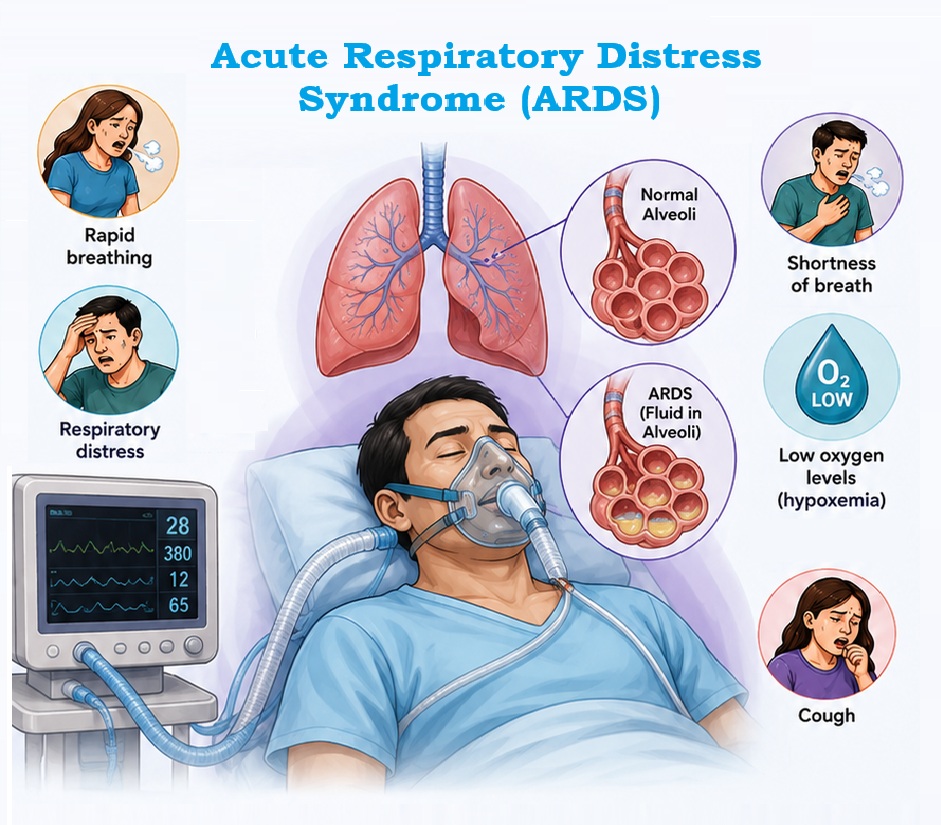
1. Early (Prodromal) Phase: Hours 0–24
The onset of ARDS is acute, typically evolving within 72 hours of the precipitating insult (by definition). Early manifestations include:
- Progressive dyspnea and tachypnea, often initially attributed to the underlying cause
- Increased work of breathing with accessory muscle recruitment, nasal flaring, and intercostal recession
- Tachycardia and hypoxemia with SpO₂ <94% on room air
- The hallmark finding: hypoxemia disproportionately refractory to supplemental oxygen — the clinician provides FiO₂ and oxygenation fails to respond as expected, reflecting intrapulmonary shunt rather than simple hypoventilation
- Dry cough; bibasal crackles on auscultation
- The patient may be diaphoretic and appear visibly distressed
2. Established Phase: Hours 24–72 and Beyond
As alveolar flooding progresses:
- Severe hypoxemia dominates — PaO₂/FiO₂ ratio falls below 300 mmHg (the threshold for ARDS diagnosis)
- Respiratory rate increases to 30–40 breaths per minute; patients are unable to maintain adequate ventilation without mechanical support
- Central cyanosis becomes apparent
- Auscultation reveals diffuse crackles and reduced air entry at bases
- Most patients require endotracheal intubation and invasive mechanical ventilation within 24–72 hours of symptom onset
- Chest radiograph demonstrates bilateral, diffuse, patchy alveolar infiltrates
- CT thorax shows the characteristic dependent consolidation with ground-glass opacities, air bronchograms, and the dorsal-to-ventral gradient of increasing density
3. Severe and Late Presentations
In patients with severe ARDS (PaO₂/FiO₂ <100 mmHg):
- Deep sedation and neuromuscular blockade may be required to facilitate lung-protective ventilation
- Signs of right ventricular strain — raised JVP, hepatomegaly, peripheral edema — reflect pulmonary hypertension and acute cor pulmonale
- Multiorgan dysfunction is common: acute kidney injury (AKI), hepatic dysfunction, encephalopathy, and cardiovascular compromise co-occur in a substantial proportion
- Patients may develop ventilator-induced lung injury if not managed with appropriate lung-protective strategies
4. Systemic Inflammatory Features
Because ARDS frequently occurs in the context of sepsis or systemic inflammatory response syndrome (SIRS), features of the underlying cause may dominate:
- Fever or hypothermia
- Hypotension, vasodilatory shock
- Altered consciousness, encephalopathy
- Signs of the precipitating condition (e.g., peritonism in abdominal sepsis, burns, trauma)
5. Long-Term Sequelae: Post-Intensive Care Syndrome (PICS)
Survivors of ARDS face a prolonged recovery trajectory. The Post-Intensive Care Syndrome (PICS) encompasses:
- Pulmonary impairment: Persistent reduction in diffusing capacity (DLCO), restrictive or obstructive spirometric defects, exercise intolerance — most improve over 6–12 months but may persist at 5 years in severe cases
- Cognitive dysfunction: Deficits in memory, attention, executive function, and processing speed — detectable in up to 70–100% of survivors at hospital discharge and persisting in 20–45% at 1 year
- Psychiatric morbidity: Post-traumatic stress disorder (PTSD), depression, and anxiety affect 20–40% of survivors, significantly impairing quality of life
- Physical rehabilitation needs: Profound ICU-acquired weakness, sarcopenia, and reduced exercise capacity necessitate structured rehabilitation
- Fatigue: Persistent fatigue is reported by the majority of survivors at 12 months
Risk Factors of Acute Respiratory Distress Syndrome (ARDS)
Acute Respiratory Distress Syndrome (ARDS) risk factors are conventionally divided into direct (pulmonary) and indirect (extrapulmonary) causes, reflecting the route by which injury reaches the alveolar-capillary membrane.
A. Direct Pulmonary Risk Factors
These conditions injure the alveolar epithelium from the airway side:
- Pneumonia (bacterial, viral, fungal): The most common cause of ARDS globally. Community-acquired pneumonia caused by Streptococcus pneumoniae, Staphylococcus aureus, and influenza virus; hospital-acquired pneumonia from Gram-negative organisms; and COVID-19 pneumonitis (a major cause of ARDS during the pandemic)
- Aspiration of gastric contents: Gastric acid and particulate matter cause direct chemical injury and secondary bacterial pneumonitis
- Pulmonary contusion: Traumatic injury to lung parenchyma, particularly following high-energy blunt chest trauma
- Inhalation injury: Smoke, toxic fumes (chlorine, phosgene, ammonia), near-drowning with aspiration
- Reperfusion injury: Post-lung transplantation primary graft dysfunction
B. Indirect (Extrapulmonary) Risk Factors
These conditions injure the alveolar-capillary membrane via the bloodstream:
- Sepsis: The most common overall cause of ARDS (accounting for ~40% of cases). The systemic inflammatory cascade directly damages pulmonary endothelium. Patients with septic shock carry an approximately 40% risk of developing ARDS.
- Major trauma and hemorrhagic shock: Activates systemic SIRS and coagulopathy
- Acute pancreatitis: Inflammatory mediators from the retroperitoneum enter the systemic circulation; severe acute pancreatitis carries a 10–25% ARDS risk
- Massive transfusion and Transfusion-Related Acute Lung Injury (TRALI): Donor antibodies reactive against recipient neutrophils or HLA antigens, or bioactive lipids in stored blood products
- Cardiopulmonary bypass: Post-pump syndrome with systemic inflammatory activation
- Drug overdose and toxin exposure: Heroin, cocaine, salicylates, paraquat
- Burns: Particularly inhalation injury combined with systemic burn response
- Traumatic brain injury: Neurogenic pulmonary edema via catecholamine surge
C. Predisposing Host Factors
Host susceptibility modifies the risk of ARDS given equivalent exposures:
- Chronic alcohol use disorder — impairs alveolar macrophage function and glutathione reserves, increasing risk approximately two-fold
- Hypoalbuminemia and nutritional deficiency — reduce oncotic pressure and antioxidant defense
- Genetic polymorphisms in inflammatory mediator genes (e.g., IL-6, ACE, TNF-α)
- Older age, obesity (particularly as a risk for COVID-19 ARDS and aspiration)
- Immunocompromised state — post-transplantation, HIV, hematological malignancy (though clinical presentation may be atypical)
- Cigarette smoking — chronic lung injury and impaired mucociliary clearance
Diagnosis of Acute Respiratory Distress Syndrome (ARDS)
A. The Berlin Definition (2012)
The Berlin Definition, developed by a task force under the European Society of Intensive Care Medicine and endorsed by the ATS and SCCM, defines ARDS by four criteria that must ALL be fulfilled:
| Criterion | Requirement |
|---|---|
| Timing | Acute onset within 1 week of a known clinical insult or new/worsening respiratory symptoms |
| Chest Imaging | Bilateral opacities on chest radiograph or CT — not fully explained by effusions, lobar/lung collapse, or nodules |
| Origin of Edema | Respiratory failure not fully explained by cardiac failure or fluid overload; requires objective assessment (e.g., echocardiography) if no risk factor present |
| Oxygenation | PaO₂/FiO₂ ratio on PEEP or CPAP ≥5 cmH₂O within one of three severity categories |
B. Berlin Severity Classification
| Category | PaO₂/FiO₂ Ratio | Hospital Mortality |
|---|---|---|
| Mild | 201–300 mmHg | ~27% |
| Moderate | 101–200 mmHg | ~32% |
| Severe | ≤100 mmHg | ~45% |
PEEP ≥5 cmH₂O is required for all categories. Mild ARDS allows non-invasive ventilation (NIV/CPAP). Moderate and severe require invasive mechanical ventilation in most cases.
C. Clinical Assessment
History and exposure assessment should identify the precipitating cause (pulmonary vs. extrapulmonary) and establish the timeline of symptom onset relative to the insult. Key clinical information includes:
- Onset and rapidity of dyspnea progression
- Recent hospitalization, procedures, transfusions, drug exposures
- Signs and symptoms of infection (fever, productive cough, urinary symptoms, abdominal pain)
- Aspiration risk (altered consciousness, vomiting, enteral feeding)
- Trauma mechanism, burn exposure, smoke inhalation
- Immune status (transplant medications, chemotherapy, HIV)
Physical examination findings include:
- Tachypnea (RR >30/min), use of accessory muscles
- Diffuse bilateral coarse crackles; reduced air entry in dependent zones
- Signs of underlying cause (wound, rash, peritonism, signs of aspiration)
- Cardiovascular assessment to exclude cardiogenic pulmonary edema (elevated JVP, S3 gallop, peripheral edema — though these may coexist)
D. Arterial Blood Gas (ABG) Interpretation
ABG analysis is essential for ARDS diagnosis and severity classification:
- Hypoxemia with PaO₂ markedly reduced relative to FiO₂ (PaO₂/FiO₂ <300)
- Respiratory alkalosis early (hyperventilation-driven CO₂ washout)
- Mixed respiratory and metabolic acidosis in severe disease — elevated lactate from systemic hypoperfusion, CO₂ retention as respiratory muscles fatigue
- Elevated A-a gradient (>150 mmHg on room air), reflecting impaired gas exchange
- PaO₂/SpO₂ ratio can serve as a non-invasive surrogate in resource-limited settings (SpO₂/FiO₂ <235 correlates with PaO₂/FiO₂ <200)
E. Chest Imaging
Plain chest radiograph (CXR):
- Bilateral alveolar opacities ("white-out"), often with air bronchograms
- The pattern is diffuse and symmetric, though it can be patchy and asymmetric
- Cardiomegaly and cephalization of vessels (as seen in cardiogenic pulmonary edema) are absent
- A ratio of the width of the vascular pedicle <65 mm supports a non-cardiogenic etiology
CT Thorax: Not required for diagnosis but provides superior characterization:
- Dependent (dorsal) consolidation, non-dependent ground-glass opacities, and a gravitational gradient — pathognomonic of ARDS
- Identifies complications: pneumothorax, pleural effusion, pulmonary embolism
- Quantifies recruitable lung volume — useful to guide PEEP titration in severe cases
- Identifies atypical or alternative diagnoses
F. Additional Investigations
- Echocardiography (bedside TTE/TOE): Mandatory if cardiogenic pulmonary edema cannot be excluded. Evaluates LV and RV function, valvular disease, and volume status. In ARDS, LV function is typically preserved. Also essential for detecting acute cor pulmonale.
- Full blood count, C-reactive protein, procalcitonin: Assess for infection and inflammatory burden
- Blood cultures, sputum/BAL cultures: Identify causative organisms in infectious ARDS
- Bronchoalveolar lavage (BAL): Neutrophilia >60% in BAL fluid is consistent with ARDS; also identifies infectious pathogens and can exclude eosinophilic pneumonia or diffuse alveolar hemorrhage
- Lactate, coagulation panel, renal and hepatic function: Assess for multiorgan dysfunction
- Pro-BNP: Elevated values raise the possibility of a cardiac contribution; however, significantly elevated pro-BNP can also occur in sepsis-associated ARDS
- Lung ultrasound: Point-of-care lung ultrasound shows B-lines (indicating alveolar-interstitial syndrome), consolidation, and pleural effusion, and can be used serially for monitoring
Differential Diagnosis of Acute Respiratory Distress Syndrome (ARDS)
| Condition | Distinguishing Features |
|---|---|
| Cardiogenic pulmonary edema | Elevated JVP, S3, PCWP >18 mmHg, cardiomegaly, responds to diuresis; LV dysfunction on echo |
| Acute interstitial pneumonias (AIP/DAD) | Subacute onset, UIP/NSIP pattern on CT, absence of precipitating risk factor |
| Eosinophilic pneumonia | Peripheral eosinophilia, BAL eosinophilia >25%, responds rapidly to steroids |
| Diffuse alveolar hemorrhage (DAH) | Hemoptysis, bloody BAL, hemosiderin-laden macrophages; associated with vasculitis or coagulopathy |
| Cryptogenic organizing pneumonia (COP) | Subacute onset; peripheral, peribronchovascular consolidation on CT; responds to steroids |
| Pulmonary embolism with infarction | Pleural-based infiltrates, hypoxemia, pleuritic pain; CT pulmonary angiogram diagnostic |
| COVID-19 ARDS | Bilateral GGOs with peripheral distribution; distinct inflammatory phenotype with coagulopathy |
Complications of Acute Respiratory Distress Syndrome (ARDS)
Acute Respiratory Distress Syndrome (ARDS) is associated with significant multiorgan morbidity, reflecting both the severity of the underlying inflammatory process and the consequences of intensive care management. 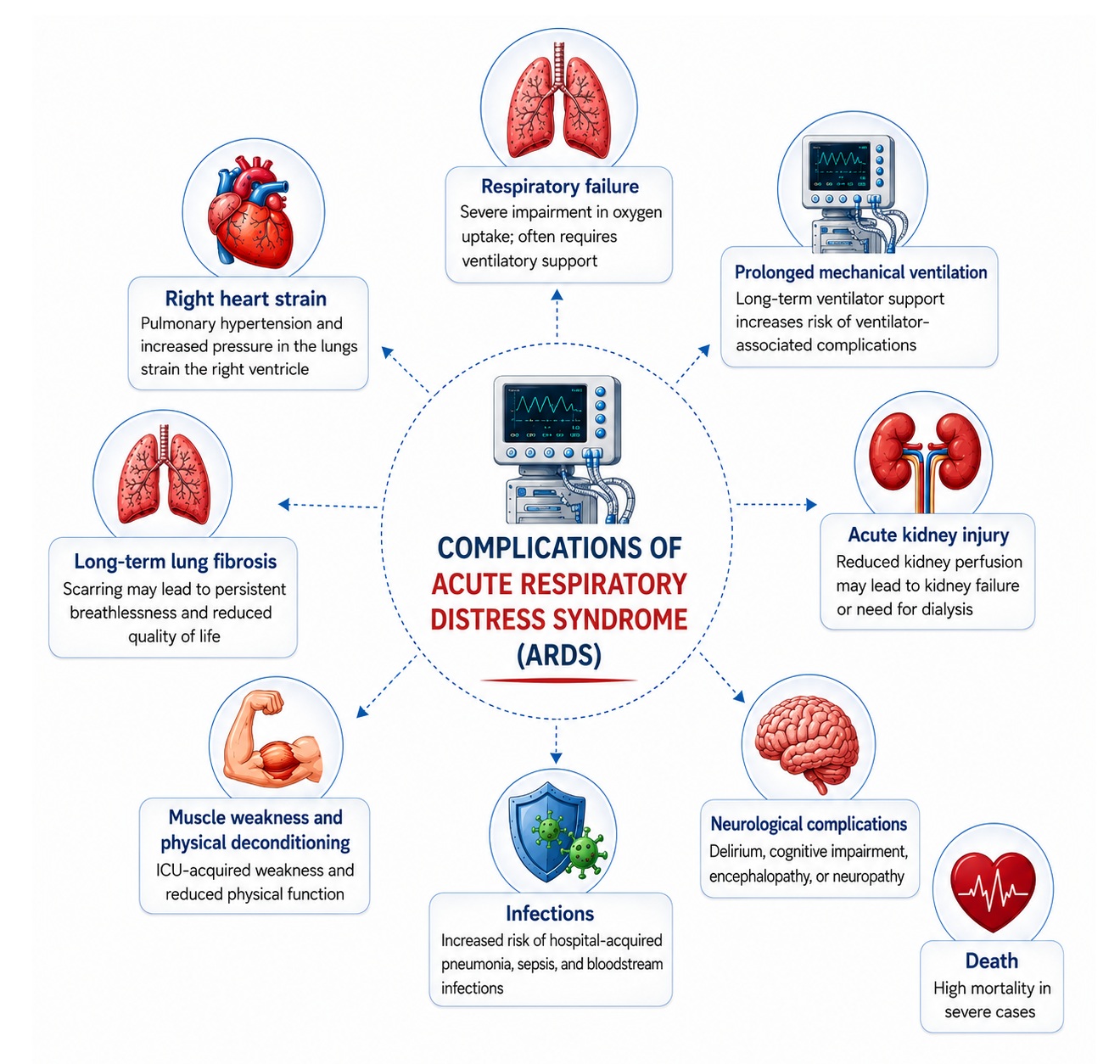
1. Ventilator-Induced Lung Injury (VILI)
Mechanical ventilation — though life-saving — can itself worsen lung injury through several mechanisms:
- Volutrauma: Overdistension of aerated alveoli from excessive tidal volumes
- Barotrauma: Pressure-related injury; clinically manifest as pneumothorax, pneumomediastinum, or subcutaneous emphysema
- Atelectrauma: Cyclic opening and closing of unstable alveoli generating shear stress at the interface between aerated and collapsed regions
- Biotrauma: Mechanical stretch-induced cytokine release perpetuating systemic inflammation
2. Acute Kidney Injury (AKI)
AKI occurs in 40–55% of patients with ARDS and represents the most common extrapulmonary organ dysfunction. It arises from hemodynamic compromise, inflammation-mediated tubular injury, and — critically — the adverse renal effects of mechanical ventilation (increased positive intrathoracic pressure reducing renal venous return and activating the renin-angiotensin system). Patients requiring renal replacement therapy face substantially higher mortality.
3. Acute Cor Pulmonale and Right Ventricular Failure
Pulmonary hypertension in ARDS imposes acute pressure overload on the right ventricle. Acute cor pulmonale — defined by RV dilatation with paradoxical septal motion on echocardiography — occurs in approximately 22–25% of moderate-to-severe ARDS and is independently associated with increased mortality. High PEEP and permissive hypercapnia (which causes pulmonary vasoconstriction) may exacerbate RV afterload.
4. Infectious Complications
Immunosuppression from critical illness, prolonged invasive ventilation, and impaired mucociliary clearance significantly increase infection risk:
- Ventilator-associated pneumonia (VAP): Occurs in approximately 28% of intubated ARDS patients; diagnosed when new or progressive infiltrates are accompanied by systemic inflammatory features after ≥48 hours of ventilation
- Catheter-related bloodstream infections (CRBSI): From central venous access
- Fungal infections: Particularly Candida and Aspergillus in immunocompromised patients
- Clostridioides difficile colitis: From broad-spectrum antibiotic use
5. Gastrointestinal Complications
Critical illness and mechanical ventilation increase risk of:
- Stress ulceration and gastrointestinal hemorrhage (mitigated with proton pump inhibitors)
- Ileus and enteral feed intolerance
- Hepatic dysfunction from systemic inflammation and hypoperfusion
6. Neurological Complications
- ICU-acquired delirium: Affects the majority of mechanically ventilated patients; associated with prolonged sedation, immobility, sleep deprivation, and medications
- Critical illness polyneuropathy and myopathy (CIPNM): Axonal degeneration and myopathic changes arising from systemic inflammation, immobility, corticosteroids, and neuromuscular blocking agents; manifests as profound, prolonged weakness following extubation
- Cognitive impairment: As detailed under long-term sequelae
7. Thrombotic Complications
ARDS, particularly in the context of sepsis or COVID-19, is associated with a hypercoagulable state:
- Deep vein thrombosis (DVT) and pulmonary embolism
- Disseminated intravascular coagulation (DIC)
- Pulmonary microvascular thrombosis — contributing directly to dead space and gas exchange impairment
Treatment of Acute Respiratory Distress Syndrome (ARDS)
Management of ARDS requires a systematic, evidence-based approach in an ICU setting. Treatment addresses three concurrent priorities: managing the underlying precipitant, supporting gas exchange without causing additional lung injury, and preventing and treating complications.
A. Treating the Underlying Cause
Identifying and aggressively treating the precipitating condition is the single most important determinant of ARDS outcome. This includes:
- Early, appropriate broad-spectrum antimicrobial therapy in sepsis-associated ARDS, guided by cultures and local resistance patterns
- Source control in abdominal sepsis (drainage, surgical debridement)
- Specific management of aspiration, pancreatitis, toxin exposure, or TRALI
B. Lung-Protective Mechanical Ventilation (The ARDSnet Protocol)
Lung-protective ventilation (LPV) is the most important and mortality-reducing intervention in ARDS, established by the landmark ARMA trial (NEJM, 2000), which demonstrated a 22% relative reduction in mortality with low tidal volume ventilation.
Core LPV parameters:
| Parameter | Target |
|---|---|
| Tidal volume (Vt) | 6 mL/kg predicted body weight (PBW) (may be reduced to 4 mL/kg if needed) |
| Plateau pressure (Pplat) | ≤30 cmH₂O |
| Driving pressure (ΔP = Pplat – PEEP) | <15 cmH₂O (driving pressure may be the optimal ventilatory target) |
| Respiratory rate | 14–35 breaths/min, adjusted to maintain pH ≥7.25 |
| PEEP | Individualized; minimum 5 cmH₂O; typically 8–15 cmH₂O in moderate-severe ARDS |
| FiO₂ | Titrated to maintain SpO₂ 88–95% or PaO₂ 55–80 mmHg |
Predicted body weight calculation:
- Males: PBW (kg) = 50 + 2.3 × [height (inches) – 60]
- Females: PBW (kg) = 45.5 + 2.3 × [height (inches) – 60]
Note: Tidal volumes must be based on PBW (reflecting lung size), NOT actual body weight.
Permissive Hypercapnia: Low tidal volumes inevitably reduce minute ventilation, allowing PaCO₂ to rise. This is generally well-tolerated, targeting a pH ≥7.20–7.25. Permissive hypercapnia should be avoided in raised intracranial pressure, severe pulmonary hypertension, and acute right heart failure.
3. PEEP Optimization
Adequate PEEP prevents end-expiratory alveolar collapse and reduces atelectrauma. However, excessive PEEP causes overdistension and impairs right ventricular function. PEEP titration strategies include:
- FiO₂/PEEP tables (ARDSnet): Standardized tables linking FiO₂ to minimum required PEEP
- Decremental PEEP trial: Lung recruitment maneuver followed by stepwise reduction in PEEP while monitoring compliance and oxygenation to identify optimal PEEP (best compliance)
- Transpulmonary pressure monitoring: Using esophageal manometry to measure pleural pressure and guide individualized PEEP in the presence of elevated chest wall compliance (obesity, abdominal hypertension)
- Electrical impedance tomography (EIT): Emerging bedside tool allowing real-time visualization of tidal ventilation distribution to optimize PEEP
4. Prone Positioning
Prone positioning is the most impactful rescue intervention for moderate-severe ARDS (PaO₂/FiO₂ <150 mmHg). The landmark PROSEVA trial (Guérin et al., NEJM 2013) demonstrated a 16% absolute reduction in 28-day mortality with early, prolonged (≥16 hours/day) prone positioning versus supine positioning in severe ARDS (NNT ~6).
Mechanisms of benefit:
- Recruitment of dorsal (previously dependent, consolidated) lung segments
- Redistribution of ventilation toward previously non-dependent lung, reducing V/Q mismatch
- Improved drainage of secretions
- Reduction in pleural pressure gradient — homogenizing stress and strain distribution
- Reduction in acute cor pulmonale by improving oxygenation-driven pulmonary vasoconstriction
Practical considerations: Requires a coordinated team of at least 3–5 staff for safe turns. Contraindications include recent open abdominal or thoracic surgery, unstable spinal injury, and open facial wounds. Complications include pressure injuries, endotracheal tube displacement, and facial edema.
5. Fluid Management
Conservative fluid management — guided by the FACTT trial (NEJM 2006) — reduces the duration of mechanical ventilation and ICU length of stay compared to a liberal fluid strategy, without increasing non-pulmonary organ failure. The target is euvolemia or mild negative fluid balance in patients who have been adequately resuscitated:
- Guided by mean arterial pressure (MAP), urine output, and dynamic indices of preload responsiveness (pulse pressure variation, stroke volume variation)
- Vasopressors are preferred over volume loading once adequate resuscitation is achieved
- Excessive fluid worsens alveolar edema, increases pulmonary hydrostatic pressure, and impairs gas exchange
6. Neuromuscular Blockade (NMB)
Early, short-course cisatracurium (48 hours) was shown to reduce mortality and improve oxygenation in moderate-severe ARDS in the ACURASYS trial (Papazian et al., NEJM 2010). However, the subsequent ROSE trial (NEJM 2019), which used lighter sedation protocols in the control arm, did not demonstrate a survival benefit for routine NMB. Current practice reserves NMB for patients with severe ventilator dyssynchrony refractory to deep sedation, or to facilitate lung-protective ventilation (controlling Pplat). Cisatracurium (organ-independent Hofmann elimination) is preferred to avoid drug accumulation in multiorgan failure.
7. Corticosteroids
The role of corticosteroids in ARDS has been debated for decades. Current evidence supports:
- Dexamethasone: The DEXA-ARDS trial (Villar et al., Lancet Respiratory Medicine 2020) showed that dexamethasone (20 mg IV daily for 5 days, then 10 mg daily for 5 days) significantly reduced 60-day mortality and ventilator-free days in moderate-severe ARDS. It is the best-supported corticosteroid regimen at present.
- Methylprednisolone: Evidence from the LaSRS trial and subsequent meta-analyses supports a benefit in early-moderate ARDS; its role in late (>14 days) fibroproliferative ARDS remains contested, with concern about harm from the original ARDS Network study.
- COVID-19 ARDS: Dexamethasone 6 mg daily for 10 days became a standard of care following the RECOVERY trial, reducing mortality in patients requiring supplemental oxygen or mechanical ventilation.
- Corticosteroids are contraindicated or require careful risk-benefit assessment in patients with active fungal infection, uncontrolled diabetes, recent gastrointestinal hemorrhage, or immunosuppression-related opportunistic infections.
8. Vasopressor and Hemodynamic Support
The majority of ARDS patients, particularly those with sepsis-associated ARDS, require vasopressor support:
- Norepinephrine is the first-line vasopressor, targeting MAP ≥65 mmHg (or higher in chronic hypertension)
- Vasopressin may be added as a second agent to reduce norepinephrine requirements
- Dobutamine for right or left ventricular dysfunction with low cardiac output
- Target perfusion adequacy: lactate clearance >10% per 2-hour interval; urine output >0.5 mL/kg/hr
9. Extracorporeal Membrane Oxygenation (ECMO)
Venovenous ECMO (VV-ECMO) provides extracorporeal gas exchange in patients with severe ARDS refractory to optimal conventional therapy, allowing extreme lung-protective ventilation ("ultra-protective ventilation") with very low tidal volumes and driving pressures.
- The CESAR trial (Peek et al., Lancet 2009) demonstrated improved survival with transfer to an ECMO center versus conventional management.
- The EOLIA trial (Combes et al., NEJM 2018) randomized severe ARDS patients to early ECMO vs. conventional ventilation; while the primary endpoint (60-day mortality) was not statistically significant, the control arm had a high crossover rate to ECMO, and a subsequent Bayesian analysis suggests a clinically meaningful benefit.
- ECMO is indicated when PaO₂/FiO₂ <80 mmHg on FiO₂ >0.8 with Pplat >30 cmH₂O after optimal ventilatory management, or when adequate ventilation cannot be maintained. It requires a highly specialized team and is associated with significant complications (hemorrhage, thrombosis, infection).
10. Adjunctive and Investigational Therapies
- Inhaled nitric oxide (iNO) and inhaled prostacyclin: Pulmonary vasodilators that selectively reduce V/Q mismatch by vasodilating ventilated lung regions. Both improve oxygenation transiently (10–20% improvement in PaO₂/FiO₂) but have not been shown to reduce mortality in randomized trials. They are used as rescue therapy for refractory hypoxemia or acute cor pulmonale while planning definitive interventions (prone positioning, ECMO).
- Recruitment maneuvers (RM): Sustained inflation (40 cmH₂O for 40 seconds) or incremental PEEP steps to open collapsed alveoli. The ART trial (JAMA 2017) demonstrated harm from aggressive RMs combined with high PEEP, cautioning against routine use. Individualized use in carefully selected patients with significant recruitability remains an option.
- High-frequency oscillatory ventilation (HFOV): Once used in severe ARDS, but the OSCAR and OSCILLATE trials demonstrated no benefit and possible harm; no longer routinely recommended.
- Mesenchymal stem cell therapy: Phase I/II trials demonstrate safety and potential anti-inflammatory benefit; Phase III trials are ongoing.
- Vitamin C and thiamine: Based on the Marik protocol rationale; large RCTs (CITRIS-ALI, VITAMINS) have not demonstrated clear clinical benefit; not currently recommended outside of clinical trials.
- Anticoagulation: Nebulized heparin and other anti-fibrinolytic strategies are under investigation in ARDS with significant intravascular coagulopathy, particularly COVID-19-associated ARDS.
11. Sedation and Analgesia
A structured approach to sedation (ABCDEF bundle) is central to ICU management:
- Analgesia-first strategy: Pain addressed before sedation (fentanyl, morphine, acetaminophen)
- Targeted light sedation using the RASS scale (target RASS –1 to 0) in stable patients not requiring NMB; reduces duration of ventilation, delirium, and ICU-acquired weakness
- Daily spontaneous awakening trials (SAT) and spontaneous breathing trials (SBT): Early liberation from mechanical ventilation when criteria are met
- Propofol and dexmedetomidine are preferred sedative agents for short-to-medium term sedation; benzodiazepines increase delirium risk and should be minimized
- Delirium management: Regular CAM-ICU assessment; non-pharmacological interventions (early mobilization, sleep hygiene, reorientation) are the cornerstone; antipsychotics have not demonstrated mortality benefit
12. Nutritional Support
Early enteral nutrition (within 24–48 hours of ICU admission) is recommended:
- Gastric or post-pyloric feeding, preferring the enteral route over parenteral whenever feasible
- Adequate protein delivery (1.2–2.0 g/kg/day) to reduce catabolism and preserve muscle mass
- Prone positioning complicates enteral feeding; most guidelines permit continued feeding in prone patients with vigilance for intolerance
- Omega-3 fatty acid supplementation initially appeared promising but was not supported by subsequent RCTs
Prevention and Control of Acute Respiratory Distress Syndrome (ARDS)
A. Prevention of Precipitating Conditions
The most effective strategy for ARDS prevention is reducing exposure to its key risk factors:
- Sepsis prevention: Hand hygiene, infection control, antimicrobial stewardship, vaccination programs (influenza, pneumococcal, COVID-19)
- Aspiration prevention: Head-of-bed elevation ≥30°, appropriate sedation management, oral decontamination in ventilated patients, careful enteral feeding protocols
- TRALI prevention: Leukocyte-reduced blood products, preferential use of male-donor or never-pregnant female-donor fresh frozen plasma, exclusion of high-risk donors
- Lung-protective intraoperative ventilation: Emerging evidence suggests that LPV during general anesthesia (Vt 6–8 mL/kg PBW, PEEP 5–8 cmH₂O) reduces postoperative pulmonary complications and ARDS incidence, particularly in high-risk surgeries (esophagectomy, cardiac surgery)
2. Early Clinical Recognition
Given that time-sensitive intervention substantially improves outcomes, healthcare systems should prioritize early recognition of at-risk patients:
- Protocol-driven screening in the emergency department and surgical wards for patients with known ARDS risk factors and new respiratory symptoms
- Rapid arterial blood gas analysis and chest imaging in deteriorating patients
- Early escalation to critical care teams for patients with PaO₂/FiO₂ <300 mmHg
3. Preventive Lung Strategies in the ICU
For patients already receiving mechanical ventilation for other indications:
- Maintain LPV parameters (Vt ≤8 mL/kg PBW, Pplat ≤28 cmH₂O) as default
- Minimize unnecessary fluid administration
- Extubate early when clinically appropriate to reduce VAP risk
4. Post-ICU Rehabilitation
Structured follow-up programs addressing the physical, cognitive, and psychological sequelae of ARDS and critical illness are essential:
- ICU follow-up clinics: Provide comprehensive assessment and coordinate rehabilitation referrals
- Pulmonary rehabilitation: Improves exercise capacity and quality of life in survivors with persistent pulmonary impairment
- Neuropsychological rehabilitation: Cognitive training and psychological support for PICS
- Peer support and survivorship programs: ARDS survivor networks and support groups reduce psychological morbidity
Prognosis of Acute Respiratory Distress Syndrome (ARDS)
The prognosis of ARDS has improved steadily since the 1990s, attributable largely to the adoption of lung-protective ventilation and better ICU supportive care. Overall ICU mortality is approximately 35–45%, with significant variation by severity:
- Mild ARDS: ~27% hospital mortality
- Moderate ARDS: ~32% hospital mortality
- Severe ARDS: ~45% hospital mortality
The cause of death in ARDS is most commonly multiorgan failure and the underlying precipitating condition (e.g., refractory septic shock), rather than refractory respiratory failure alone — a finding that underscores the importance of aggressive management of the underlying cause.
Prognostically favorable factors: Younger age, absence of comorbidities, direct pulmonary cause (vs. sepsis), lower severity scores (APACHE II, SOFA), response to prone positioning, early enrollment in ECMO centers when indicated.
Prognostically adverse factors: Advanced age, chronic liver failure, hematological malignancy, immunosuppression, high driving pressure, non-response to recruitment, multiorgan dysfunction on admission, and persistent elevation of inflammatory biomarkers.
Survivors face a protracted recovery: up to 5 years may be required to approach baseline pulmonary function, and cognitive and psychological morbidity may persist indefinitely in a significant proportion.
Frequently Asked Questions on Acute Respiratory Distress Syndrome (ARDS)
1. How does ARDS differ from cardiogenic pulmonary edema?
Both conditions cause bilateral pulmonary infiltrates and hypoxemia. The key distinction lies in mechanism: cardiogenic pulmonary edema results from elevated pulmonary capillary hydrostatic pressure (left ventricular failure or volume overload), whereas ARDS reflects increased alveolar-capillary permeability driven by inflammation. Clinically, cardiogenic edema is associated with elevated JVP, S3 gallop, peripheral edema, cardiomegaly on CXR, and elevated pro-BNP, and responds to diuresis. ARDS is associated with a precipitating insult, preserved LV function on echocardiography, and hypoxemia refractory to supplemental oxygen.
2. What is the correct way to calculate tidal volume in ARDS?
Tidal volume must be calculated using predicted body weight (PBW), not actual body weight. This is because PBW reflects lung size, and obese patients should not receive larger tidal volumes simply because they weigh more. A 120 kg obese patient with a height of 170 cm has a PBW of approximately 65 kg, and should receive Vt 6 mL/kg × 65 = 390 mL — not 720 mL based on actual body weight. This error is a common and clinically significant mistake.
3. When should prone positioning be initiated?
Prone positioning is indicated early (within 12–36 hours of ARDS onset) in patients with moderate-severe ARDS (PaO₂/FiO₂ ≤150 mmHg on FiO₂ ≥0.6 and PEEP ≥5 cmH₂O), based on the PROSEVA trial protocol. Early initiation is critical — prone positioning initiated late in the disease course has not been shown to be beneficial. Sessions should last ≥16 hours/day.
4. Are steroids beneficial in ARDS?
Yes, in certain contexts. Current evidence most strongly supports dexamethasone (per the DEXA-ARDS protocol) in moderate-severe ARDS not caused by COVID-19, and dexamethasone 6 mg for 10 days in COVID-19 ARDS (RECOVERY trial). The greatest caution applies to patients with active fungal infection, uncontrolled sepsis without adequate source control, and the late fibroproliferative phase, where steroid benefit is less certain.
5. What is driving pressure and why is it important?
Driving pressure (ΔP) is defined as plateau pressure minus PEEP (Pplat − PEEP), and represents the dynamic stress applied to the respiratory system with each tidal breath. It is a surrogate for the tidal strain delivered to the aerated lung volume. A driving pressure >15 cmH₂O has been consistently and independently associated with increased ARDS mortality in retrospective analyses, and targeting ΔP <15 cmH₂O — rather than targeting Vt or Pplat alone — may be the most physiologically appropriate ventilatory objective.
6. What are the indications for ECMO in ARDS?
VV-ECMO should be considered in severe ARDS meeting the following criteria despite optimal conventional therapy (≥16 hours prone, optimized PEEP, neuromuscular blockade): PaO₂/FiO₂ <80 mmHg on FiO₂ ≥0.8, or pH <7.20 with PaCO₂ >60 mmHg despite maximal ventilatory support, with a potentially reversible cause. Contraindications include advanced chronic pulmonary disease, non-recoverable multiorgan failure, and inability to anticoagulate. ECMO should be managed in specialist centers with adequate case volumes.
7. How should oxygenation targets be set in ARDS?
Target SpO₂ 88–95% (PaO₂ 55–80 mmHg), not supranormal values. Hyperoxia generates ROS, worsens atelectasis through absorption of oxygen, and is independently associated with increased ICU mortality. The HOT-ICU trial (NEJM 2021) found no significant mortality difference between a PaO₂ target of 60 mmHg vs. 90 mmHg, but supported avoiding hyperoxia.
8. Can ARDS be diagnosed without mechanical ventilation?
Under the original Berlin Definition, all ARDS severity categories require PEEP or CPAP ≥5 cmH₂O. However, early or mild ARDS may be managed with high-flow nasal oxygen (HFNO) or non-invasive ventilation (NIV), both of which can provide a degree of functional PEEP. In resource-limited settings, a modified Kigali definition omitting the oxygenation criterion (replacing ABG with SpO₂/FiO₂ ratio) and chest imaging criterion has been validated.
References
- Ashbaugh DG, Bigelow DB, Petty TL, Levine BE. Acute respiratory distress in adults. Lancet. 1967;2(7511):319–323.
- ARDS Definition Task Force; Ranieri VM, Rubenfeld GD, et al. Acute respiratory distress syndrome: the Berlin Definition. JAMA. 2012;307(23):2526–2533.
- The Acute Respiratory Distress Syndrome Network (ARDSnet). Ventilation with lower tidal volumes as compared with traditional tidal volumes for acute lung injury and the acute respiratory distress syndrome. N Engl J Med. 2000;342(18):1301–1308.
- Guérin C, Reignier J, Richard JC, et al. Prone positioning in severe acute respiratory distress syndrome. N Engl J Med. 2013;368(23):2159–2168.
- Papazian L, Forel JM, Gacouin A, et al. Neuromuscular blockers in early acute respiratory distress syndrome. N Engl J Med. 2010;363(12):1107–1116.
- National Heart, Lung, and Blood Institute ARDS Clinical Trials Network; Wiedemann HP, Wheeler AP, Bernard GR, et al. Comparison of two fluid-management strategies in acute lung injury. N Engl J Med. 2006;354(24):2564–2575.
- Villar J, Ferrando C, Martínez D, et al. Dexamethasone treatment for the acute respiratory distress syndrome: a multicentre, randomised controlled trial. Lancet Respir Med. 2020;8(3):267–276.
- Combes A, Hajage D, Capellier G, et al. Extracorporeal membrane oxygenation for severe acute respiratory distress syndrome. N Engl J Med. 2018;378(21):1965–1975.
- Peek GJ, Mugford M, Tiruvoipati R, et al. Efficacy and economic assessment of conventional ventilatory support versus extracorporeal membrane oxygenation for severe adult respiratory failure (CESAR). Lancet. 2009;374(9698):1351–1363.
- Bellani G, Laffey JG, Pham T, et al. Epidemiology, patterns of care, and mortality for patients with acute respiratory distress syndrome in intensive care units in 50 countries. JAMA. 2016;315(8):788–800.
- Herridge MS, Tansey CM, Matté A, et al. Functional disability 5 years after acute respiratory distress syndrome. N Engl J Med. 2011;364(14):1293–1304.
- RECOVERY Collaborative Group; Horby P, Lim WS, Emberson JR, et al. Dexamethasone in hospitalized patients with Covid-19. N Engl J Med. 2021;384(8):693–704.
- Ferguson ND, Fan E, Camporota L, et al. The Berlin definition of ARDS: an expanded rationale, justification, and supplementary material. Intensive Care Med. 2012;38(10):1573–1582.
- Gattinoni L, Pesenti A. The concept of "baby lung." Intensive Care Med. 2005;31(6):776–784.
- Amato MB, Meade MO, Slutsky AS, et al. Driving pressure and survival in the acute respiratory distress syndrome. N Engl J Med. 2015;372(8):747–755.