











Gout – Uric acid Analysis
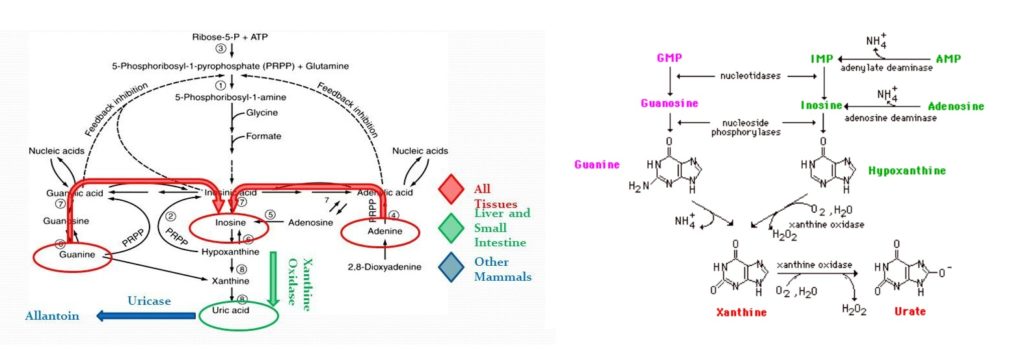
Uric acid is a non-protein nitrogenous waste product of the body, derived from purines of the diet. Purines are the end products of nucleoprotein digestion ( high in red meat). The two purines found in RNA and DNA are adenine and guanine. The first step in the catabolism of purines is their hydrolytic deamination to form xanthine and hypoxanthine. These are then oxidized to uric acid. Uric acid is eliminated by the body through the kidney. Uric acid is filtered in the glomeruli and partially reabsorbed by the tubules and it is excreted in urine. In Kidney disorders, as with other non-protein nitrogen fractions of the plasma, uric acid builds up in the body.
- Plasma or serum : 3.5 to 7.2 mg/dl ( Phosphotungstate method )
- Urine (24 hour ) : Average diet: 500 mg/day
- High purine diet : 1 g/day
- (Conversion to International
The quantity excreted in urine, depends to a large extent, on the purine content of the diet and normally the excretion rate is 0.5-2.0 g/24 hrs. The normal plasma uric acid level is 2.0-7.0 mg/dl. The uric acid concentration in erythrocytes is lower than in plasma so that the normal range in whole blood is 1-4 mg/dl. The plasma uric acid level is little affected by variation in the purine content of the diet and maintains a steady state between endogenous synthesis and urinary excretion.
A raised plasma uric acid level is found in several renal and prerenal conditions like Gout, Renal failure, Leukemia, Polycythemia, Keto-acidosis, Lactate excess, Chronic lead nephropathy etc. Decreased level of uric acid is found where Renal tubular defect ( Fanconi's syndrome & Wilsons disease), administration of ACTH, Galactosemia, Heavy metal Poisoning and also drugs such as aspirin, corticosteroids, allopurinol and probenecid cause low serum uric acid levels. Hyperuricemia is most commonly defined by serum or plasma uric acid concentrations greater than 7.0 mg/dl in men and above 6.0 mg/dl in women. All the manifestations resulting from hyperuricemia are due to the low solubility of the uric acid in water.
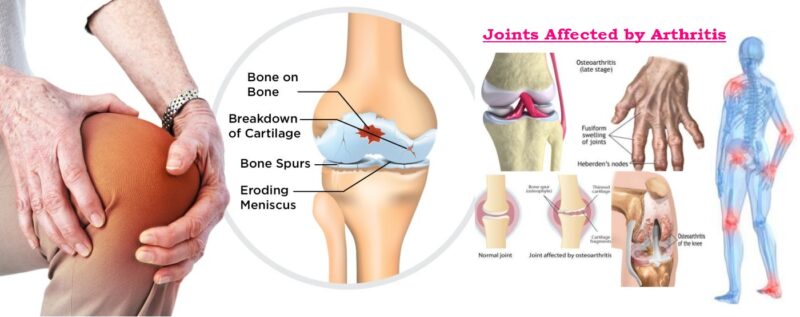
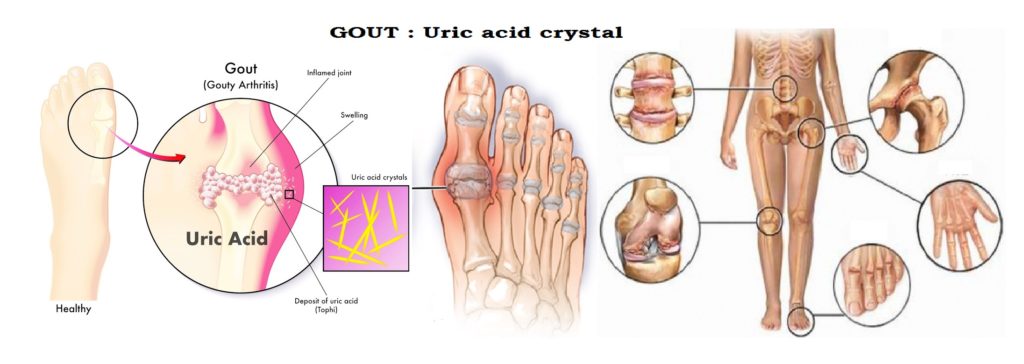
Gout is associated with hyperuricemia. In Gout, monosodium Urate crystal precipitate from supersaturated body fluids. Gouty arthritis maybe associated with Urate
crystals deposited in joint fluid, in tissues surrounding the joint and also in other soft tissues and they elicit an intense inflammatory response consisting of polymophonuclear leukocytes & macrophages. Gout is a type of inflammatory arthritis that causes sudden severe attacks of pain, swelling, warm and redness in the joints. Gout typically affects the big toe & other joints; the premier stage of gout affect only one joint, but as the disease becomes more severe, it can affect several joints at the same time, if untreated, joint damage can occur. Increased excretion of uric acid may cause uric acid crystals to be deposited in the collecting tubules & lower urinary tract leading to calculi or stone formation with renal damage. Several risk factors of Gout are as follows :
- Gender: Men get more susceptible to gout more than women and they tend to be diagnosed at younger ages than women. Women are more likely to experience gout after menopause. Gout is rare in children, unless they have an inherited genetic disorder that predisposes them to gout.
- Obesity: Being overweight or having metabolic syndrome is associated with gout.
- Diet: A diet high in fructose, meat (especially red meat and organ meat), some types of seafood and excessive alcohol consumption (especially beer and spirits) increases your risk of gout.
- Concurrent diseases: Medical conditions such as diabetes, high blood pressure, high cholesterol, and chronic kidney disease are associated with an increased risk of gout. Medications used to treat some of these conditions also affect blood levels of uric acid. Joint trauma or surgery can evoke a gout.
Primary Gout :
Most cases of this type are due to increased synthesis of purine nucleotides. It may be due to any one of the following reasons-
- Abnormality in 5-phosphoribosyl aminotransferase activity, which is the rate limiting enzyme of uric acid synthesis.
- Abnormality in phosphoribosyl pyrophosphate which is the ribose-5- phosphate donor for the de novo synthesis.
- Deficiency of enzyme of salvage pathway: The recycling of purines formed by degradation of nucleotides in vivo is achieved by salvage pathway. The key reactant in this pathway is PRPP. Deficiency of enzymes in this pathway results in increased availability of PRPP and decreased level of inhibitory purine nucleotides.
- Glucose-6-Phosphatase deficiency: In this condition, glucose -6-phosphate can't be converted to glucose. Hence more glucose is channeled into the pentose phosphate pathway. This results in increased availability of ribose -5-phosphate which leads to increased formation of PRPP. In addition accumulation of lactic acid, decreases uric acid excretion.
- Glutathione reductase variant with increased activity: The abnormality in this enzyme leads to increased production of ribose-5-phosphate and thereby increased level of PRPP.
Secondary Gout :
It may be caused by reduced urinary excretion rate due to :
- Renal failure
- Lactic acid acidosis and ketoacidosis lactic acid and ketoacidosis interfere with uric acid excretion).
- Treatment with thiazide diuretics which inhibit tubular secretion of uric acid.
- Hypertension and preeclamptic toxemia.
- Secondary gout may also be caused due to increased turnover rate of nucleic acid. This may be observed in :
- Rapidly growing malignant cells, eg., leukemias, lymphomas, polycythemia.
- Increased tissue breakdown after treatment of large malignant tumors.
- Increased tissue damages due to trauma and raised rate of catabolism as in starvation.
 Important Information :
Important Information :
- Gouty attacks may be precipitated by high purine diet and increased intake of alcohol. Increased intake of alcohol leads to accumulation of lactic acid.
- Lesch -Nyhan syndrome is a rare x-linked inherited disorder of purine metabolism result from total or partial deficiency of HGPRTase ( Hypoxanthine guanine phosphoribosyl transferase) which catalyzes following reaction. The result is accumulation of PRPP leading to excessive synthesis of uric acid.

Determination of Uric Acid by Enzymatic (Uricase) method
Determination of Uric acid is carried out by two methods - Uricase method (the enzymatic method) and the Phosphotungstate method. The enzymatic method is more specific & sensitive for determination of true uric acid level. This method can be used on photometer, spectrophotometer, Semi and Fully automated analyzers; hence it followed by the routine laboratories in developing countries.
Principle :
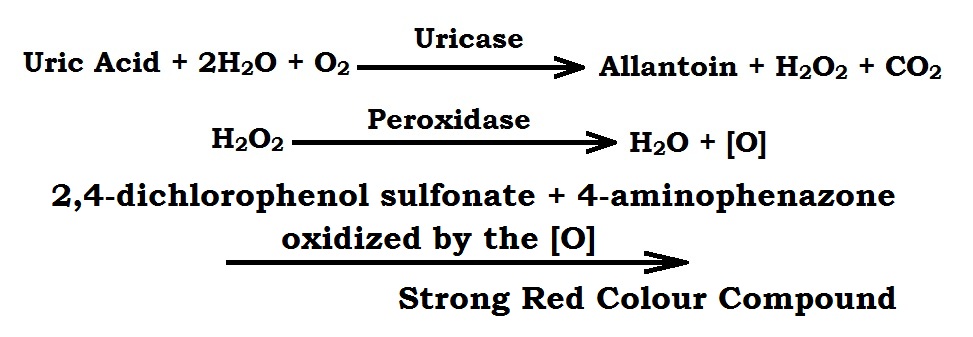
Uric acid is catalyze by uricase enzyme in the presence of water and oxygen (air) to Allantoin with the formation of hydrogen peroxide. This H2O2 further split into H2O & [O] in presence of peroxides enzyme. The phenolic chromogens present in the reagent 2,4-dichlorophenol sulfonate and 4-aminophenazone get oxidized by the [O] to form a strong red colour compound. The intensity of the produced color is directly proportional to the concentration of uric acid present in the specimen which is measured by the photometer at 510 nm (500-530 nm, green filter).
Reagent & Requirement :
- Stock regent in the lyophilized form contains the following :
- Buffer, pH : 7.5 : 100 mmol/L
- Uricase : 100 IU/L
- Peroxidase : 140 IU/L
- Chromogen : 2.5 µmol/L
- Surfactants / Stabilizers
- Uric acid Standard : 5.0 mg/dl (The reagents are stable at 2-8°C)
Preparation of working reagent : Working reagent is prepared by mixing contents of stock lyophilized reagent with distilled water. Working reagent is stable at 2-8°C for 60 days.
- Test tubes and racks.
- Pasteur Pipettes
- Graduated pipette.
- Micropipette with tips.
- Colorimeter machine.
- Incubator machine.
Normal Value :
- Male : 3.2 - 7.2 mg/dl
- Female : 2.0 -6.0 mg/dl
(Possible panic range of serum Uric acid is >12 mg/dl)
Procedure :
- All the reagents are brought to the room temperature before the test.
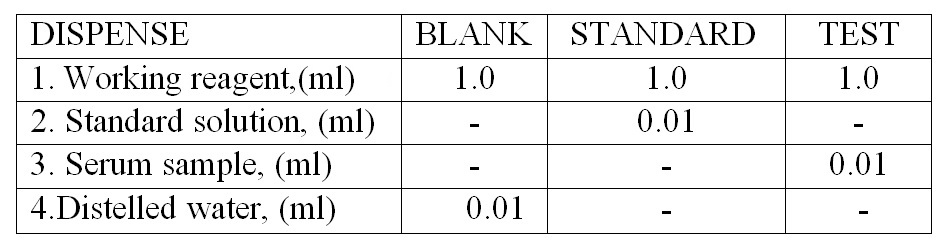
- Three dry and clean test tubes are taken and marked as Blank (B), Standard (S), and Test (T).
- Dispense the Working reagent, Uric acid Standard, Distilled water & Serum in the above mention test tube respectively.
- Then mixed well. Incubated at 37°C for 5 minutes or room temperature for 10 minutes.
- The absorbance of the Test and Standard are measured against Blank in the colorimeter at 510 nm (500-530 nm, green filter).
- Standard concentration may be selected as per the absorbance of the test in case of higher absorbance of the test in case of higher absorbance higher concentration is taken.
- Calculations :

Special Note :
- The method is linear upto 25 mg/dl.
- Glucose, bilirubin, ascorbic acid, urea, proteins and haemoglobin etc. do not interfere in this test in moderate concentrations.
- For the determination of urine Uric acid, dilute the specimen 1:10 in distilled water and perform the test.