











Hepatitis B – Sign & Symptoms, Transmission, Risk factors, Diagnosis, Complication, Treatment and Prevention
Hepatitis B is a potentially life-threatening liver infection caused by the Hepatitis B virus (HBV), a partially double-stranded DNA virus belonging to the family *Hepadnaviridae*, genus *Orthohepadnavirus*. It is one of the most prevalent infectious diseases worldwide and represents a major global public health burden. The WHO estimates that approximately 296 million people are living with chronic HBV infection globally, with approximately 1.5 million new infections annually and approximately 820,000 deaths per year from hepatitis B-related complications, including cirrhosis and hepatocellular carcinoma (HCC). Hepatitis B has a global distribution, with the highest endemic burden in sub-Saharan Africa and the Western Pacific Region.
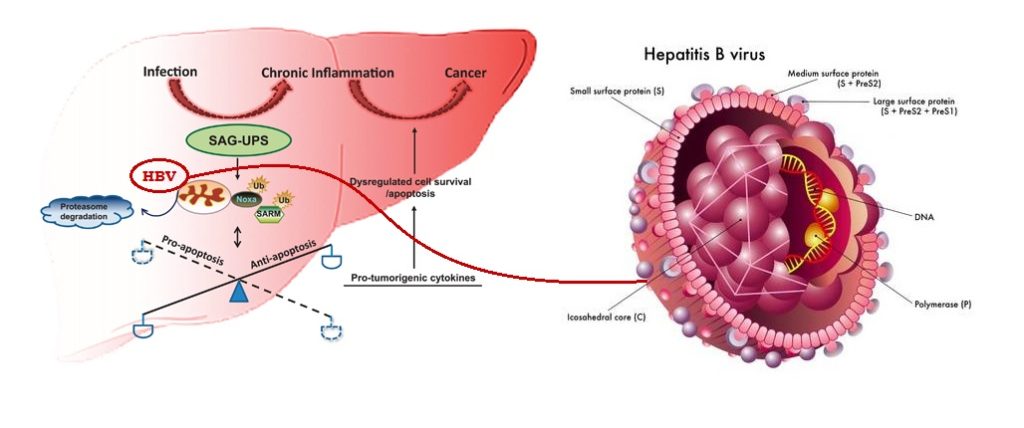
HBV is 50–100 times more infectious than HIV and can survive outside the body on environmental surfaces for at least 7 days. The virus is transmitted through contact with infectious blood and body fluids, including through sexual intercourse, sharing of contaminated needles and syringes, mother-to-child transmission during childbirth, and contact with blood or open sores of infected individuals. The hepatitis B genome encodes four overlapping reading frames producing the surface antigens (HBsAg — the outer envelope glycoprotein used as the primary diagnostic marker), core/precore antigens (HBcAg/HBeAg), polymerase (reverse transcriptase with RNase H activity), and the X protein (HBx — transcriptional transactivator involved in oncogenesis). 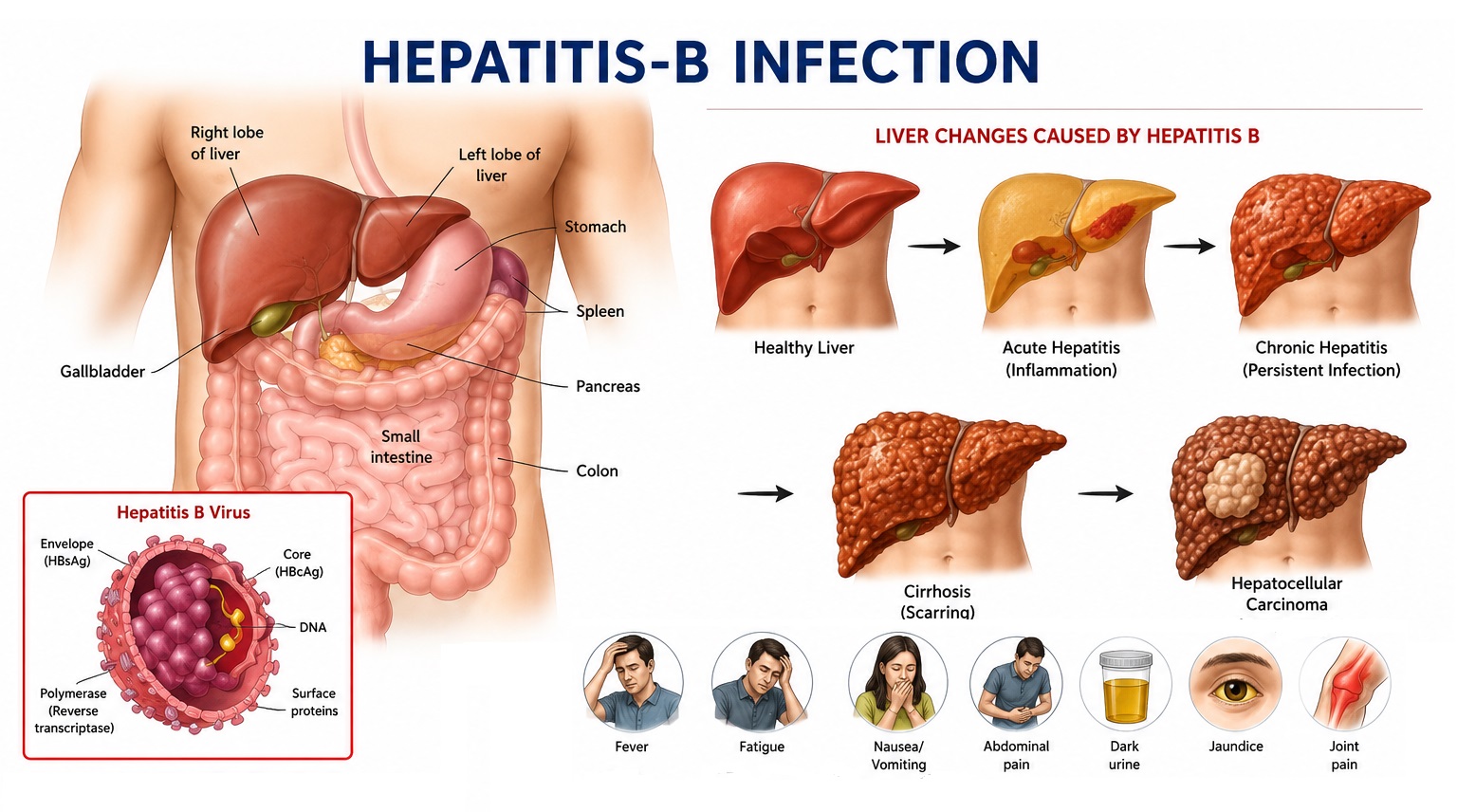
The pathophysiology of hepatitis B liver injury is predominantly immune-mediated rather than directly cytopathic. HBV infects hepatocytes through binding of the pre-S1 region of the large surface protein to the sodium-taurocholate cotransporting polypeptide (NTCP) receptor. Following entry, the viral genome circularizes to form covalently closed circular DNA (cccDNA) — an episomal minichromosome that serves as the transcriptional template for all viral RNAs and persists in infected hepatocytes for the lifetime of the cell, explaining the impossibility of complete viral eradication with current therapies and the risk of reactivation. HBV-specific CD8+ cytotoxic T lymphocytes (CTLs) are the primary effectors of hepatocyte destruction; in chronic HBV, viral persistence drives CTL exhaustion and immune tolerance, allowing ongoing viral replication without effective immune clearance.
Sign and Symptoms of Hepatitis B
The clinical presentation of hepatitis B spans a wide spectrum from asymptomatic infection to fulminant hepatic failure. The course is profoundly influenced by the age at acquisition — perinatal infection leads to chronic disease in >90% of cases, while adult-acquired infection is self-limiting in >95% — and by the phase of the host-virus immune interaction.
A. Acute Hepatitis B
The incubation period of acute HBV ranges from 30 to 180 days (average 60–90 days), during which the patient is asymptomatic but HBsAg is detectable and the individual is infectious.
1. Prodromal Phase (1–2 Weeks Before Jaundice)
- Serum Sickness-Like Syndrome: Approximately 10–20% of patients with acute HBV develop an immune complex-mediated prodrome before jaundice, characterized by arthralgias (particularly small joints), arthritis, urticarial or maculopapular rash (from circulating HBsAg-anti-HBs immune complexes), fever, and malaise. This prodrome is mediated by HBsAg-containing immune complexes activating complement and triggering type III hypersensitivity.
- Constitutional Symptoms: Profound fatigue, malaise, anorexia, nausea, and low-grade fever are the dominant symptoms of the prodromal phase.
- Right Upper Quadrant Discomfort: Dull or aching pain in the right upper quadrant or epigastrium reflects hepatic capsular distension from hepatic inflammation and early hepatomegaly.
2. Icteric Phase (2–8 Weeks)
- Jaundice: Scleral icterus (yellow discoloration of the whites of the eyes) followed by frank jaundice (yellow skin discoloration) results from elevation of both conjugated and unconjugated bilirubin — the former from impaired hepatocytic bilirubin excretion, the latter from haemolysis and reduced hepatocytic uptake.
- Dark Urine (Bilirubinuria): Conjugated bilirubin — water-soluble — appears in the urine before jaundice is clinically apparent, producing dark, cola-coloured urine. This is often the first sign noticed by the patient.
- Pale Stools (Acholia): Reduced bilirubin excretion into the bile produces pale, clay-coloured stools from absence of stercobilin.
- Pruritus: Generalised itching results from accumulation of bile acids in the skin, stimulating cutaneous sensory nerve fibres.
- Tender Hepatomegaly: Physical examination reveals an enlarged, smooth, tender liver with a sharp edge. Splenomegaly is present in approximately 10–15% of cases.
3. Recovery Phase
Most immunocompetent adults (>95%) clear HBV spontaneously within 4–6 months. Clinical symptoms resolve, liver enzymes normalize, HBsAg clears, and protective anti-HBs antibodies appear, conferring lifelong immunity. Resolution is confirmed by seroconversion from HBsAg-positive to anti-HBs-positive.
B. Fulminant Hepatitis B
Approximately 0.5–1% of patients with acute HBV develop fulminant hepatic failure (FHF) — a catastrophic form of acute hepatitis characterized by massive hepatic necrosis and rapid deterioration in liver function within 8 weeks of the onset of jaundice. Clinical features include:
- Deepening jaundice with coagulopathy (PT prolongation >5 seconds above control)
- Hepatic encephalopathy: Progressive alteration of consciousness from confusion and personality change to stupor and coma (Grades I–IV), resulting from accumulation of ammonia, aromatic amino acids, and neurotoxic substances from the failing liver
- Cerebral oedema: Elevated intracranial pressure causing headache, vomiting, Cushing's triad, and uncal herniation
- Acute kidney injury from hepatorenal syndrome
- Coagulopathy with multiorgan bleeding
- Hypoglycaemia
- FHF from acute HBV carries 70–80% mortality without liver transplantation
C. Chronic Hepatitis B
Chronic HBV infection — defined as persistence of HBsAg for more than 6 months — is a dynamic disease progressing through distinct immunological phases:
- Immune Tolerant Phase : Common in perinatally infected individuals. Characterized by very high HBV DNA levels (>10⁷ IU/mL), HBeAg positivity, normal or minimally elevated ALT, minimal liver inflammation on biopsy, and high infectivity. Immune tolerance reflects neonatal immune immaturity and impaired HBV-specific T-cell responses induced by perinatal antigen exposure.
- Immune Active (Immune Clearance) Phase : The immune system begins attacking HBV-infected hepatocytes, producing fluctuating or persistently elevated ALT, significant liver inflammation and fibrosis progression, and declining HBV DNA. This phase may last years and is characterized by repeated episodes of hepatic flares.
- Immune Control (Inactive Carrier) Phase : Following HBeAg seroconversion (loss of HBeAg, appearance of anti-HBe), many patients enter a phase of viral suppression with HBV DNA <2,000 IU/mL, normal ALT, and minimal hepatic inflammation. Inactive carriers have a low risk of disease progression but require lifelong monitoring for reactivation.
- HBeAg-Negative Chronic Hepatitis B : A proportion of patients develop HBeAg-negative chronic hepatitis with pre-core or basal core promoter mutations that prevent or reduce HBeAg production while maintaining viral replication. This phase is characterized by fluctuating HBV DNA (usually 2,000–20,000 IU/mL), intermittent ALT elevation, and ongoing hepatic inflammation and fibrosis — often progressing to cirrhosis insidiously.
Symptoms of Chronic HBV:
- Most patients are asymptomatic for decades
- Fatigue, right upper quadrant discomfort, and anorexia are the most common non-specific complaints
- Extrahepatic manifestations: polyarteritis nodosa (PAN), membranous glomerulonephritis, cryoglobulinaemia — mediated by circulating immune complexes
- Manifestations of cirrhosis (if advanced): ascites, peripheral oedema, jaundice, spider naevi, palmar erythema, gynaecomastia, caput medusae, variceal bleeding, hepatic encephalopathy
Risk Factors of Hepatitis B
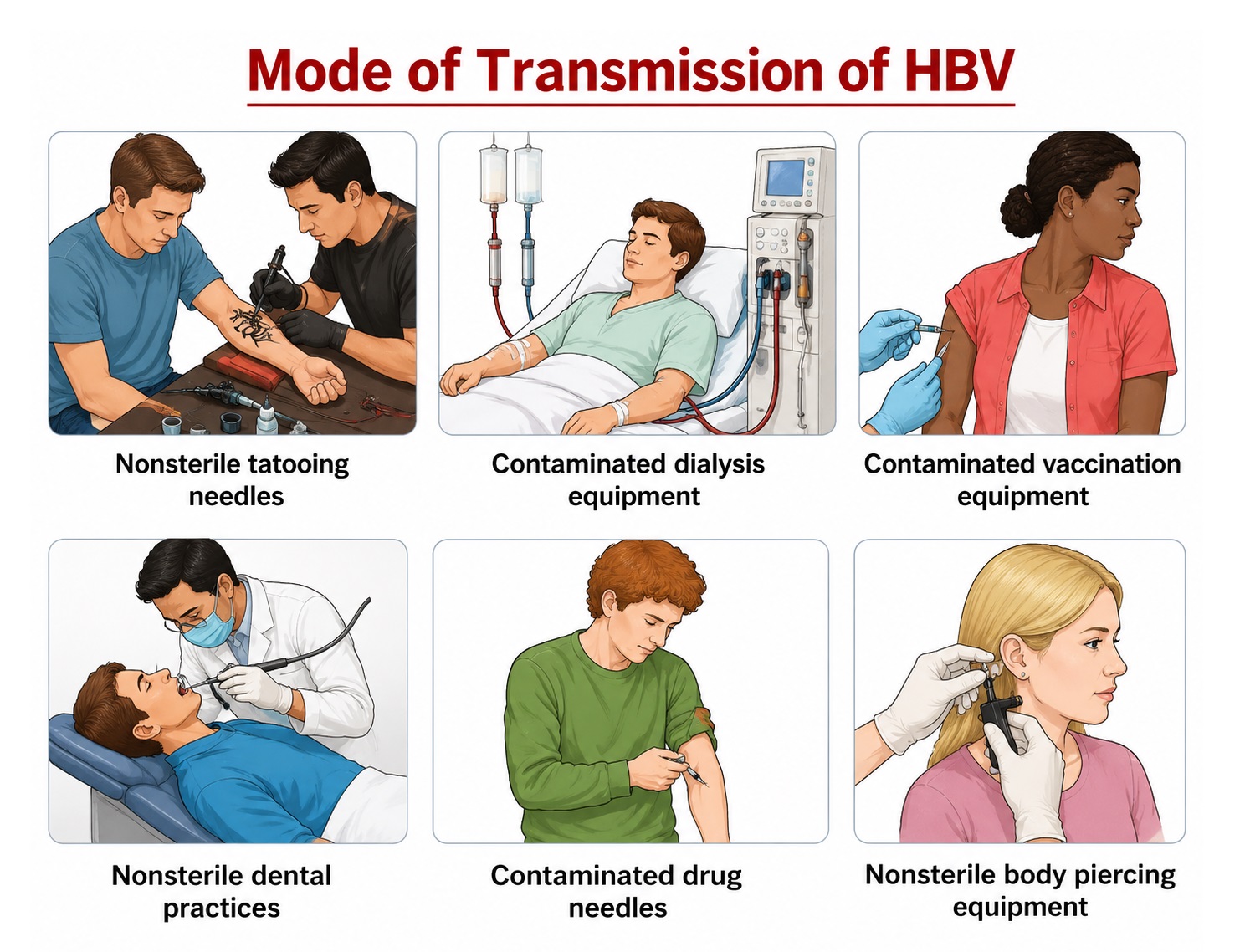
A. Parenteral and Blood-Borne Transmission
- Injection Drug Use: Sharing of needles, syringes, and drug paraphernalia among people who inject drugs (PWID) is the most important HBV transmission route in high-income countries with low perinatal transmission due to universal infant vaccination. HBV can survive on surfaces and in dried blood for up to 7 days.
- Needlestick and Sharps Injuries: Healthcare workers face a 6–30% risk of HBV infection following a single needlestick injury from an HBeAg-positive source patient (compared to 0.3% for HIV). This underscores the critical importance of HBV vaccination for all healthcare workers.
- Blood Transfusion and Blood Products: Before universal blood donor screening was implemented, HBV transmission via transfusion was common. In countries with rigorous screening programs, this route has been effectively eliminated, but remains a risk in settings with inadequate blood safety infrastructure.
- Unsafe Medical Procedures: Reuse of needles and syringes in medical care without adequate sterilization, unsafe injection practices, and unsterilized dental or surgical equipment are significant HBV transmission routes in resource-limited settings.
B. Sexual Transmission
Sexual intercourse — particularly unprotected anal intercourse (which carries the highest risk), vaginal intercourse with an infected partner, and multiple sexual partnerships — is a major route of HBV transmission. The risk of HBV transmission per sexual encounter from an HBeAg-positive partner is approximately 10–20% for receptive anal intercourse, significantly higher than for most other sexually transmitted infections. HBV is present in semen, vaginal secretions, and saliva.
C. Vertical (Mother-to-Child) Transmission
Vertical transmission from an HBV-infected mother to her newborn during childbirth is the most important route of HBV transmission globally, particularly in Asia, and is the primary driver of the large chronic HBV burden in the Western Pacific Region. The risk of perinatal transmission is approximately:
- 70–90% from HBeAg-positive, high viral load mothers (HBV DNA >200,000 IU/mL) without prophylaxis
- 10–30% from HBeAg-negative mothers without prophylaxis
- <5% with appropriate immunoprophylaxis (birth dose HBV vaccine + HBIG) plus maternal antiviral therapy
Transmission occurs predominantly during delivery through exposure to maternal blood and genital secretions; intrauterine infection is rare. Breastfeeding does not significantly increase transmission risk when the infant has received appropriate prophylaxis.
D. Other Risk Factors
- Household Contact: Non-sexual household contact with a chronically infected individual — through shared razors, toothbrushes, or other blood-contaminated items — carries a risk of HBV transmission.
- Tattoos and Body Piercing: Performed with non-sterile equipment in unregulated settings.
- Haemodialysis: Renal dialysis patients face elevated HBV exposure risk from blood-contaminated surfaces and equipment, particularly in facilities without adequate infection control.
- Men Who Have Sex with Men (MSM): Higher risk from sexual practices and multiple partners.
- Travel to High-Endemicity Regions: Without vaccination, travel to areas with high HBV prevalence increases exposure risk.
Diagnosis of Hepatitis B
Diagnosis of HBV infection requires serological testing to detect viral antigens and host antibodies, molecular testing to quantify viral replication, and assessment of hepatic inflammation and fibrosis to stage disease severity and guide treatment decisions.
1. Clinical Examination
- Assessment of Liver Disease Severity : Physical examination in suspected chronic HBV should systematically evaluate for stigmata of chronic liver disease: jaundice, scleral icterus, spider naevi (>5 above the nipple line suggests significant liver disease), palmar erythema, Dupuytren's contracture, leukonychia, clubbing, hepatomegaly (right lobe involvement, firm consistency), splenomegaly (portal hypertension), ascites (shifting dullness, fluid thrill), peripheral oedema, gynecomastia (in males), testicular atrophy, encephalopathy (flapping tremor, altered consciousness), and caput medusae (engorged periumbilical veins from portal hypertension).
- Extrahepatic Manifestations : Examination for extrahepatic immune complex-mediated manifestations — skin vasculitis, arthritis, peripheral neuropathy, and signs of glomerulonephritis (hypertension, oedema, haematuria) — is important in HBV management.
2. Serological Diagnosis
The serological diagnosis of HBV involves a panel of antigens and antibodies that together define the phase of infection, immune status, and treatment response:
- Hepatitis B Surface Antigen (HBsAg) : HBsAg is the first serological marker to appear after HBV infection, detectable 1–10 weeks before clinical symptoms (in the incubation period). Its persistence beyond 6 months after acute infection defines chronic HBV infection. HBsAg-positive individuals are infectious and can transmit HBV to others. HBsAg-negative individuals who are anti-HBc-positive and anti-HBs-negative may have occult HBV infection (detectable HBV DNA without HBsAg).
- Anti-HBs (Hepatitis B Surface Antibody) : Anti-HBs is a protective, neutralizing antibody that indicates:
- Recovery from acute HBV infection (anti-HBs appears as HBsAg clears — the "window period" may be weeks to months).
- Successful immunization with HBV vaccine (vaccine-induced anti-HBs without anti-HBc positivity).
- Anti-HBs titre ≥10 mIU/mL is considered protective.
- HBeAg and Anti-HBe : HBeAg is a secreted protein derived from the precore region of the HBV genome that serves as a marker of active viral replication and high infectivity. HBeAg seroconversion — disappearance of HBeAg and appearance of anti-HBe — generally indicates reduction in viral replication and is an important treatment endpoint. However, HBeAg-negative chronic hepatitis with ongoing replication (due to precore/BCP mutations) must be excluded by HBV DNA testing.
- Anti-HBc (Hepatitis B Core Antibody) :
- Anti-HBc IgM: Present in acute HBV infection and during flares of chronic HBV; useful for diagnosing acute hepatitis B when HBsAg has already been cleared (window period).
- Anti-HBc IgG (total anti-HBc): Persists lifelong after HBV exposure; indicates current or past HBV infection. Its presence without HBsAg or anti-HBs (isolated anti-HBc) may indicate occult HBV infection, false-positive result, or waning anti-HBs.
3. Molecular Diagnosis
- HBV DNA (Viral Load) : Quantitative HBV DNA measurement by real-time PCR is the most sensitive indicator of HBV replication, ranging from <10 IU/mL (lower limit of detection) to >10⁹ IU/mL in high-replication states. HBV DNA is used to:
- Confirm active viral replication and guide treatment decisions (treatment indicated when HBV DNA >2,000 IU/mL with elevated ALT/significant fibrosis).
- Monitor treatment response (viral load suppression to undetectable levels is the primary treatment target).
- Detect antiviral drug resistance (with genotypic resistance testing).
- Risk-stratify patients for HCC development.
- HBV Genotyping : Eight major HBV genotypes (A–H) have distinct geographic distributions and clinical implications regarding disease progression and treatment response. Genotype B and C predominate in Asia, with genotype C associated with higher rates of HCC. Genotype A predominates in Northern Europe and North America and has a better response to pegylated interferon therapy.
4. Assessment of Hepatic Fibrosis
Staging of hepatic fibrosis is essential for treatment decisions, as antiviral therapy is indicated in patients with significant fibrosis (Metavir F2 or above) regardless of other parameters.
- Liver Biopsy: The historical gold standard for fibrosis staging; provides histological information on inflammation (grading) and fibrosis (staging). The METAVIR score (F0–F4) and Ishak score are the most widely used histological staging systems. Limitations include sampling variability, invasiveness, and risk of bleeding.
- Transient Elastography (FibroScan): Non-invasive measurement of liver stiffness (in kilopascals) by ultrasound-mediated shear wave propagation. Provides accurate estimation of fibrosis stage and is now recommended as the preferred non-invasive fibrosis assessment tool. Liver stiffness >9.5 kPa suggests significant fibrosis; >12 kPa suggests cirrhosis.
- Serum Fibrosis Markers: APRI (AST-to-platelet ratio index) and FIB-4 index (combining age, AST, ALT, and platelet count) are simple, widely available non-invasive fibrosis scores useful in resource-limited settings.
Complications of Hepatitis B
A. Liver Cirrhosis
Approximately 15–40% of individuals with chronic HBV develop liver cirrhosis over 20–30 years of infection, characterized by progressive replacement of functional liver parenchyma with fibrotic scar tissue and regenerative nodules. Cirrhosis — particularly decompensated cirrhosis — carries a 5-year mortality of 70–80% without liver transplantation. Clinical manifestations of decompensated cirrhosis include ascites, spontaneous bacterial peritonitis (SBP), variceal haemorrhage (oesophageal or gastric varices rupture, potentially fatal), hepatic encephalopathy, hepatorenal syndrome, and coagulopathy.
B. Hepatocellular Carcinoma (HCC)
Chronic HBV infection is the single most important global risk factor for hepatocellular carcinoma, responsible for approximately 50–55% of HCC cases worldwide. HBV-related HCC may develop even in the absence of cirrhosis — a unique feature that distinguishes HBV from HCV. Mechanisms of HBV oncogenesis include: integration of HBV DNA into the host genome causing genomic instability, HBx protein-mediated transcriptional activation of oncogenes, cccDNA persistence despite antiviral therapy, and ongoing inflammation-mediated oxidative stress and hepatocyte regeneration driving mutagenesis. Annual surveillance with liver ultrasound ± serum AFP (alpha-fetoprotein) every 6 months is recommended for all cirrhotic HBV patients and for high-risk non-cirrhotic HBV patients (males >40 years with family history of HCC, elevated HBV DNA).
C. Renal Complications
HBV-associated membranous nephropathy — caused by deposition of HBsAg-containing immune complexes in the glomerular basement membrane — is the most common HBV-related renal manifestation, presenting with nephrotic syndrome (proteinuria, hypoalbuminaemia, oedema). Other glomerulonephritides (IgA nephropathy, mesangioproliferative GN) and HBV-associated polyarteritis nodosa (involving medium-sized vessels of the kidneys, causing renal ischaemia) may occur.
D. HBV Reactivation
HBV reactivation — abrupt increase in HBV replication in a patient with inactive chronic HBV or resolved HBV (anti-HBc positive) — can occur during immunosuppressive therapy (rituximab, anthracycline-based chemotherapy, steroids, anti-TNF agents), organ transplantation, or HIV co-infection. Reactivation can cause acute-on-chronic liver failure, which carries high mortality. Screening all patients for HBV markers before immunosuppression and prophylactic antiviral therapy for high-risk patients is mandatory.
Treatment of Hepatitis B
The goal of HBV treatment is to achieve sustained suppression of viral replication to undetectable HBV DNA levels, leading to normalization of liver inflammation, regression of fibrosis, prevention of cirrhosis, and reduction of HCC risk. Complete elimination of HBV (cure) is currently not achievable due to the persistence of cccDNA and integrated HBV DNA in hepatocytes. Treatment endpoints include HBeAg seroconversion (in HBeAg-positive patients), normalization of ALT, and — ideally — HBsAg loss with anti-HBs seroconversion (functional cure).
A. Indications for Antiviral Therapy
Treatment is indicated in patients with:
- HBV DNA >20,000 IU/mL (HBeAg-positive) or >2,000 IU/mL (HBeAg-negative) with elevated ALT (>2× upper limit of normal) or significant liver fibrosis (Metavir F≥2) or necroinflammation on biopsy
- Cirrhosis (compensated or decompensated) regardless of HBV DNA level
- HBV reactivation
- Pregnancy in women with high viral load (HBV DNA >200,000 IU/mL) to prevent perinatal transmission
B. Nucleos(t)ide Analogue (NUC) Therapy — First-Line
NUCs inhibit the HBV reverse transcriptase (polymerase), preventing synthesis of new viral DNA. They are orally administered, well tolerated, and require lifelong treatment in most patients (as viral relapse occurs after discontinuation in the absence of functional cure).
- Tenofovir Disoproxil Fumarate (TDF — Viread): The preferred first-line agent for most patients. High antiviral potency, high barrier to resistance, well tolerated. Renal and bone toxicity are potential long-term concerns, requiring monitoring of renal function and bone density.
- Tenofovir Alafenamide (TAF — Vemlidy): A prodrug of tenofovir with improved renal and bone safety profile compared to TDF, now preferred in patients with renal impairment or osteoporosis. Equivalent antiviral potency to TDF.
- Entecavir (ETV — Baraclude): A guanosine nucleoside analogue with high antiviral potency and high barrier to resistance (in treatment-naive patients). An alternative first-line agent; generic formulations widely available.
- Lamivudine and Adefovir: Older NUCs with low barrier to resistance; no longer recommended as first-line agents due to high rates of drug resistance.
C. Pegylated Interferon-Alpha (PegIFN-α)
Pegylated interferon-alpha (Peg-IFN-α-2a, Pegasys) provides both antiviral and immunomodulatory effects and can achieve functional cure (HBsAg loss) in a minority of carefully selected patients with a finite treatment duration (48 weeks). HBsAg loss rates are approximately 5–10% with Peg-IFN in genotype A patients (higher than with NUCs) and 1–3% in genotype C. Major limitations include subcutaneous injection, significant adverse effects (flu-like symptoms, depression, cytopenia, autoimmune disorders), and contraindications in decompensated cirrhosis, pregnancy, psychiatric illness, and autoimmune disease. Best responses are seen in patients with low HBV DNA, high ALT, HBV genotype A/B, and young age.
D. Management of Complications
- Cirrhosis and Portal Hypertension: Beta-blockers (propranolol, carvedilol) for variceal prophylaxis; endoscopic variceal ligation for large varices; diuretics (spironolactone ± furosemide) for ascites; transjugular intrahepatic portosystemic shunt (TIPS) for refractory ascites or variceal bleeding.
- HCC: Treatment modalities include surgical resection, radiofrequency ablation, transarterial chemoembolisation (TACE), selective internal radiation therapy (SIRT), sorafenib/lenvatinib (systemic therapy), and liver transplantation — guided by tumour burden and liver function (Barcelona Clinic Liver Cancer staging).
- Liver Transplantation: Indicated for decompensated cirrhosis unresponsive to antiviral therapy and for HCC meeting transplant criteria (Milan criteria). HBV recurrence post-transplantation is prevented by lifelong entecavir/TDF prophylaxis with or without hepatitis B immunoglobulin (HBIG).
Prevention of Hepatitis B
A. Vaccination — The Most Powerful Prevention Tool
The HBV vaccine is a recombinant hepatitis B surface antigen (rHBsAg) vaccine administered as a 3-dose series (0, 1, and 6 months), producing protective anti-HBs antibody titres (≥10 mIU/mL) in >95% of healthy adults. It is the first vaccine demonstrated to prevent a primary hepatocellular carcinoma. Key vaccination strategies include:
- Universal Infant Immunization: A birth dose (within 24 hours of delivery) is critical for preventing perinatal transmission, followed by 2–3 additional doses in the first 6 months. Combination vaccines (DTP-HepB-Hib) simplify immunization programs.
- Adolescent and Adult Catch-Up Vaccination: For unvaccinated individuals and those at high risk (healthcare workers, MSM, PWID, sexual contacts of HBV-infected individuals, dialysis patients, travelers to high-endemicity areas).
- Accelerated Schedule (0, 1, 2 months with booster at 12 months): For rapid protection in outbreak settings or pre-travel vaccination.
- Assessment of Vaccine Response: Post-vaccination anti-HBs testing is recommended for healthcare workers and other high-risk individuals 1–2 months after the third dose.
B. Post-Exposure Prophylaxis (PEP)
For unvaccinated individuals with significant HBV exposure (needlestick from HBsAg-positive source, sexual contact with infected individual, or neonates born to HBsAg-positive mothers):
- Hepatitis B Immunoglobulin (HBIG): Provides immediate passive immunity; administered within 12–24 hours of exposure (0.06 mL/kg IM).
- HBV Vaccine: Initiated simultaneously with HBIG at a different anatomical site and completed as a 3-dose series.
- For neonates born to HBsAg-positive mothers: HBIG (0.5 mL IM) + HBV vaccine (birth dose) within 12 hours of delivery → >90% effective in preventing perinatal transmission.
C. Prevention of Blood-Borne Transmission
- Universal blood and organ donor screening for HBsAg, anti-HBc, and HBV DNA.
- Harm reduction programs: needle and syringe exchange programs, opioid substitution therapy, and education for people who inject drugs.
- Universal precautions in healthcare settings: personal protective equipment, safe disposal of sharps, and sterilization of medical equipment.
- Safe tattooing and body piercing practices using sterile single-use equipment.
D. Prevention of Sexual Transmission
- Condom use with partners of unknown HBV status.
- HBV vaccination for all sexually active individuals not previously vaccinated.
- Partner notification and vaccination for sexual contacts of HBsAg-positive individuals.
Common FAQs on Hepatitis B
- What causes Hepatitis B?
Hepatitis B is caused by the Hepatitis B virus (HBV), a partially double-stranded DNA virus of the family Hepadnaviridae. HBV infects hepatocytes through the NTCP receptor and establishes cccDNA — a persistent viral episome in the nucleus — that underlies chronic infection. The liver damage in hepatitis B is primarily immune-mediated, caused by HBV-specific cytotoxic T lymphocytes attacking infected hepatocytes.
- How is Hepatitis B transmitted?
HBV is transmitted through contact with infectious blood, semen, vaginal secretions, and other body fluids. The primary routes are: sexual intercourse with an infected person, sharing of needles/syringes among people who inject drugs, mother-to-child transmission during childbirth, needlestick or sharps injuries in healthcare settings, and contact with blood through sharing of razors, toothbrushes, or other personal items.
- What is the difference between acute and chronic Hepatitis B?
Acute hepatitis B refers to the initial infection and the immune response to it — most adults clear the infection spontaneously within 6 months. Chronic hepatitis B is defined as persistence of HBsAg for more than 6 months. The risk of chronicity is inversely related to age at acquisition: >90% of perinatally infected infants develop chronic HBV, compared to only 5–10% of immunocompetent adults.
- What does HBsAg-positive mean?
A positive HBsAg result indicates that the person is currently infected with HBV and is infectious to others. If HBsAg remains positive for more than 6 months, the person has chronic HBV infection. HBsAg-negative individuals who are anti-HBs-positive are immune to HBV — either through vaccination or recovery from past infection.
- Can Hepatitis B be cured?
Chronic hepatitis B cannot currently be cured in the traditional sense because the virus establishes cccDNA in hepatocyte nuclei that cannot be eliminated by available antivirals. However, antiviral therapy can suppress viral replication to undetectable levels, reverse liver inflammation and fibrosis, prevent progression to cirrhosis and HCC, and in a small proportion of patients achieve "functional cure" (HBsAg loss). Research into curative strategies targeting cccDNA is ongoing.
- What is Hepatitis B e-antigen (HBeAg) and why does it matter?
HBeAg is a protein secreted by HBV-infected hepatocytes that indicates active viral replication and high infectivity. HBeAg-positive patients have very high viral loads and are highly contagious. HBeAg seroconversion (loss of HBeAg and appearance of anti-HBe antibody) indicates reduction in viral replication and is an important treatment milestone. However, HBeAg-negative chronic hepatitis can still have significant viral replication due to precore/BCP mutations.
- Who is at highest risk of Hepatitis B?
High-risk groups include: infants born to HBsAg-positive mothers (without prophylaxis), people who inject drugs, healthcare workers, individuals with multiple sexual partners, MSM, household contacts of HBsAg-positive individuals, patients on haemodialysis, and individuals in countries with high HBV endemicity.
- What is HBV reactivation?
HBV reactivation is a sudden increase in HBV replication in individuals with inactive chronic HBV or resolved HBV infection, typically triggered by immunosuppressive therapy (particularly rituximab, corticosteroids, or anthracycline-based chemotherapy). It can cause severe acute hepatitis and acute-on-chronic liver failure, potentially fatal. All patients being considered for immunosuppressive therapy should be screened for HBV markers.
- How does Hepatitis B cause liver cancer?
HBV causes hepatocellular carcinoma through multiple mechanisms: integration of HBV DNA into the host genome causing chromosomal instability, HBx protein transactivating oncogenes and suppressing tumour suppressor genes (p53), chronic inflammation driving hepatocyte regeneration and mutagenesis, and oxidative stress from immune-mediated damage. Importantly, HBV-related HCC can arise even without cirrhosis — a feature unique to HBV compared to HCV.
- Is Hepatitis B vaccine safe and effective?
The HBV vaccine is extremely safe (one of the most extensively used vaccines globally) and highly effective, producing protective antibody titres in >95% of healthy infants, children, and young adults. It is the first vaccine to prevent a human cancer (HCC). Adverse effects are generally mild (injection site pain, low-grade fever). The vaccine is based on recombinant HBsAg and contains no live virus.
- Can breastfeeding transmit Hepatitis B?
HBsAg has been detected in breast milk, but the risk of HBV transmission through breastfeeding is considered negligible when the infant has received appropriate perinatal immunoprophylaxis (birth dose HBV vaccine + HBIG within 12 hours of delivery). WHO recommends that breastfeeding should not be discouraged in HBsAg-positive mothers whose infants have received immunoprophylaxis.
- What are the treatment options for chronic Hepatitis B?
The two main treatment modalities are: nucleos(t)ide analogues (NUCs) — particularly tenofovir (TDF or TAF) and entecavir — which suppress viral replication with daily oral tablets and minimal side effects, requiring long-term or lifelong treatment; and pegylated interferon-alpha, which has immunomodulatory and antiviral effects, is administered by weekly subcutaneous injection for 48 weeks, and can achieve functional cure in a minority of patients.
- What monitoring is required in chronic Hepatitis B patients?
Patients with chronic HBV require lifelong monitoring including: 6-monthly liver ultrasound ± AFP (alpha-fetoprotein) for HCC surveillance in high-risk patients; 3–6 monthly HBV DNA, ALT, and HBeAg/anti-HBe assessment; annual liver fibrosis assessment; renal function monitoring in patients on TDF; and periodic assessment of treatment response, compliance, and potential drug resistance.
- What is occult Hepatitis B infection?
Occult HBV infection is defined as the presence of HBV DNA in serum and/or liver tissue in individuals who are HBsAg-negative. It is detected by sensitive PCR methods and may represent resolved infection with very low-level viral persistence (anti-HBc positive, anti-HBs positive or negative) or infection with HBsAg escape mutants. Occult HBV infection is clinically significant because it can reactivate during immunosuppression and can be transmitted through blood transfusion and organ donation.
- How can Hepatitis B transmission from mother to child be prevented?
Perinatal HBV transmission can be effectively prevented by: timely administration of the HBV birth dose vaccine + HBIG (hepatitis B immunoglobulin) within 12 hours of delivery (>90% effective); antiviral therapy (TDF from 28 weeks gestation) for highly viraemic mothers (HBV DNA >200,000 IU/mL); completion of the infant HBV vaccination series; and post-vaccination testing at 9–12 months to confirm infant seroprotection and maternal HBsAg-negative status.
Bibliography
- Harrison's Principles of Internal Medicine — Editors: J. L. Jameson, A. S. Fauci, D. L. Kasper, S. L. Hauser, and J. Loscalzo. Publisher: McGraw-Hill Education.
- Mandell, Douglas, and Bennett's Principles and Practice of Infectious Diseases — Editors: J. E. Bennett, R. Dolin, and M. J. Blaser. Publisher: Elsevier.
- Sleisenger and Fordtran's Gastrointestinal and Liver Disease — Editors: M. Feldman, L. S. Friedman, and L. J. Brandt. Publisher: Elsevier.
- Oxford Textbook of Medicine — Editors: J. Firth, C. Conlon, and T. Cox. Publisher: Oxford University Press.
- WHO Guidelines for the Prevention, Care and Treatment of Persons with Chronic Hepatitis B Infection — World Health Organization, Geneva.
- AASLD 2018 Hepatitis B Guidance — Authors: Terrault N. A. et al. Hepatology.
- EASL 2017 Clinical Practice Guidelines on the Management of Hepatitis B Virus Infection. Journal of Hepatology.
- Lok A. S. F. and McMahon B. J. Chronic Hepatitis B. Hepatology, 2007.
- Schweitzer A. et al. Estimations of Worldwide Prevalence of Chronic Hepatitis B Virus Infection. Lancet, 2015.
- Pol S. and Lampertico P. First-Line Treatment of Chronic Hepatitis B with Entecavir or Tenofovir. Journal of Hepatology, 2012.
- Revill P. A. et al. A Global Scientific Strategy to Cure Hepatitis B. Lancet Gastroenterology and Hepatology, 2019.
- Medical Microbiology — Authors: P. R. Murray, K. S. Rosenthal, and M. A. Pfaller. Publisher: Elsevier.
- Liang T. J. Hepatitis B: The Virus and Disease. Hepatology, 2009.
- Global Hepatitis Report 2017 — World Health Organization, Geneva.
- Sherris Medical Microbiology — Authors: K. J. Ryan and C. G. Ray. Publisher: McGraw-Hill Education.