











Heart Attack (Myocardial Infarction) – Sign and Symptoms, Risk Factors, Diagnosis, Complications, Treatment and Prevention
Heart attack, medically known as a Myocardial Infarction (MI), is a life-threatening medical emergency that occurs when blood flow to a portion of the heart muscle is severely reduced or completely blocked for long enough to cause cell death (infarction). The word myocardial refers to the heart muscle, and infarction means tissue death due to oxygen deprivation. Myocardial Infarction is an acute coronary syndrome caused by prolonged myocardial ischemia resulting from partial or complete occlusion of a coronary artery, most commonly due to atherosclerotic plaque rupture and thrombus formation. Clinically, patients present with chest pain, dyspnea, diaphoresis, and hemodynamic instability. 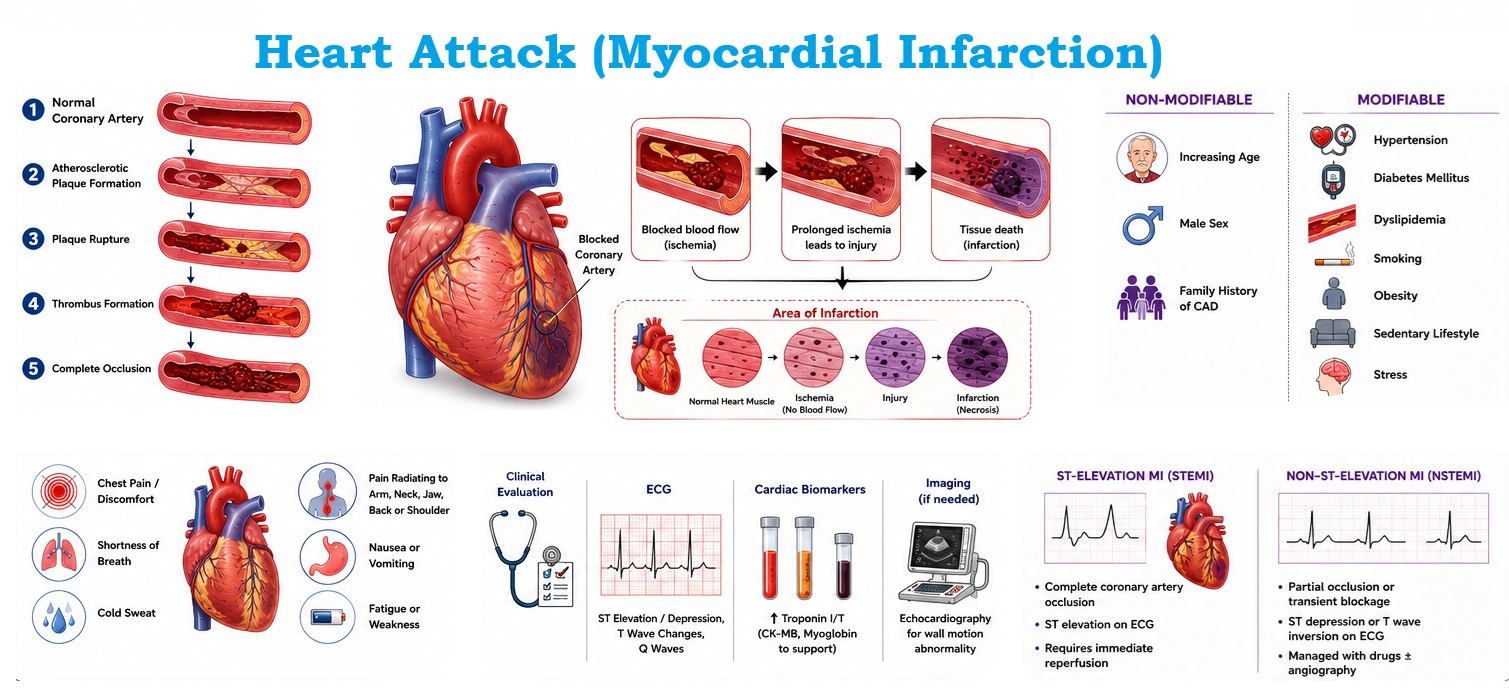
The heart is a continuously working muscle that requires a constant and rich supply of oxygen-rich blood to function properly. This supply is delivered through the coronary arteries — two main vessels that branch off the aorta and spread across the surface of the heart. When one or more of these arteries becomes blocked, the downstream heart muscle is deprived of oxygen. If the blockage is not rapidly cleared, the affected cardiac tissue begins to die within 20–40 minutes — an irreversible process that impairs the heart's ability to pump blood effectively.
Heart attacks are the leading single cause of death worldwide. According to the World Health Organization (WHO), cardiovascular diseases, predominantly heart attacks and strokes, claim approximately 17.9 million lives each year — accounting for 32% of all global deaths. Recognizing the symptoms early and seeking immediate medical care is the single most important factor in surviving and recovering from a myocardial infarction.
Causes & Mechanism of Myocardial Infarction (MI)
The vast majority of heart attacks are caused by coronary artery disease (CAD), a condition in which the arteries that supply the heart become narrowed and hardened due to a build-up of fatty plaques — a process called atherosclerosis.
Step-by-Step Pathophysiology
Less Common Causes
Coronary artery spasm (Prinzmetal's angina), spontaneous coronary artery dissection (SCAD) — more common in young women — severe anemia, cocaine or amphetamine use, and very rarely, emboli from endocarditis can also precipitate a heart attack in the absence of significant atherosclerosis.
Types of Myocardial Infarction
Cardiologists classify heart attacks based on ECG changes, the extent of heart muscle involvement, and the degree of arterial blockage:
- TEMI ST-Elevation MI : Complete artery blockage. ST-segment elevation on ECG. Full-thickness (transmural) infarction. Most severe; requires emergency reperfusion.
- NSTEMI Non–ST-Elevation MI : Partial artery blockage. No ST elevation; may show ST depression or T-wave changes. Elevated cardiac biomarkers confirm infarction.
- Silent MI : Occurs without the classic chest pain — common in diabetics and older adults. Often discovered incidentally on ECG or echocardiogram. Carries the same long-term risks.
- Unstable Angina : Part of Acute Coronary Syndrome (ACS). No biomarker elevation but similar presentation; considered a warning sign preceding a full MI.
Signs & Symptoms of Myocardial Infarction
Heart attack symptoms can vary widely — from dramatic crushing chest pain to vague discomfort or no symptoms at all. Recognizing the warning signs and acting fast can save your life.
A. Classic Symptoms of MI
- Chest Pain or Pressure — The hallmark symptom; described as tightness, squeezing, heaviness, burning, or a crushing sensation in the center or left side of the chest. May last more than a few minutes, or come and go.
- Radiation of Pain — Discomfort that spreads (radiates) to the left arm, both arms, neck, jaw, back, or upper abdomen. Left-arm pain is a classic warning sign.
- Shortness of Breath (Dyspnea) — May occur with or without chest pain; caused by reduced pumping efficiency and pulmonary congestion.
- Cold Sweat (Diaphoresis) — Profuse, clammy sweating that is not explained by heat or physical exertion — a response driven by the sympathetic nervous system.
- Nausea and Vomiting — Common, especially in inferior MI (affecting the bottom wall of the heart) due to vagal nerve stimulation.
- Dizziness or Lightheadedness — Can result from reduced cardiac output or irregular heartbeat.
- Extreme Fatigue — Particularly in women — an unusual, overwhelming tiredness that may precede the event by days or weeks.
B. Atypical Presentations
- Jaw, neck, or throat pain
- Upper abdominal pain or heartburn
- Sudden unexplained fatigue
- Palpitations or rapid heartbeat
- Anxiety or sense of impending doom
- Pain in either arm or shoulder
- Confusion (especially in elderly)
- Syncope (fainting)
Risk Factors of Myocardial Infarction
Risk factors for heart attack are divided into modifiable (can be changed or treated) and non-modifiable (fixed biological characteristics). Understanding your personal risk profile allows for targeted prevention.
| Risk Factor | Category | Risk Level | Details |
|---|---|---|---|
| Hypertension | Modifiable | Very High | Sustained high blood pressure damages arterial walls, accelerating atherosclerosis. Target BP <130/80 mmHg. |
| High LDL Cholesterol | Modifiable | Very High | LDL ("bad") cholesterol drives plaque formation. Statins reduce LDL and MI risk by 25–35%. |
| Cigarette Smoking | Modifiable | Very High | Doubles to quadruples MI risk. Toxins damage endothelium, increase clotting tendency, and reduce HDL. |
| Diabetes Mellitus | Modifiable | Very High | People with diabetes have 2–4× the MI risk. Hyperglycemia accelerates atherosclerosis and often masks symptoms (silent MI). |
| Obesity | Modifiable | High | BMI >30 is strongly linked to hypertension, dyslipidemia, and diabetes — all MI risk factors. Central (abdominal) obesity is especially dangerous. |
| Physical Inactivity | Modifiable | Moderate | Regular aerobic exercise reduces MI risk by up to 35%. Even 150 min/week of moderate-intensity activity is protective. |
| Unhealthy Diet | Modifiable | Moderate | High intake of saturated fat, trans fat, sodium, and ultra-processed foods raises LDL, BP, and inflammation. |
| Chronic Stress | Modifiable | Moderate | Elevates cortisol and adrenaline, raising BP and promoting platelet aggregation. Linked to unhealthy coping behaviors. |
| Age | Non-Modifiable | High | Risk rises sharply after age 45 in men and 55 in women (post-menopause). Older age = longer lifetime plaque accumulation. |
| Male Sex | Non-Modifiable | Moderate | Men have higher risk at younger ages. After menopause, women's risk approaches men's. Estrogen has a cardioprotective effect. |
| Family History / Genetics | Non-Modifiable | High | A first-degree relative (parent or sibling) with premature heart disease (men <55, women <65) significantly increases risk. |
| Prior MI or Angina | Non-Modifiable | Very High | Previous coronary events markedly raise the risk of recurrence. Lifelong secondary prevention therapy is essential. |
Emerging Risk Factors
Newer research also identifies sleep apnea, chronic kidney disease, autoimmune diseases (e.g., rheumatoid arthritis, lupus), air pollution exposure, periodontal (gum) disease, and psychosocial stress as independent cardiovascular risk factors receiving increasing clinical attention.
Diagnosis of Myocardial Infarction
Rapid and accurate diagnosis is critical. Emergency teams use a combination of patient history, physical examination, electrocardiography, and blood tests to confirm or rule out myocardial infarction within minutes.
Key Diagnostic Tools
1. Electrocardiogram (ECG / EKG) : The first-line investigation — results in 10 minutes. Detects ST-elevation, ST-depression, T-wave inversions, and new left bundle branch block (LBBB). Identifies infarct location and guides urgency of intervention. Serial ECGs are obtained as patterns may evolve.
2. Cardiac Biomarkers (Blood Tests) : Troponin I and T are the gold-standard biomarkers. They are released into the bloodstream when heart muscle cells are damaged. High-sensitivity troponin assays can detect elevation within 1–3 hours of onset. CK-MB (creatine kinase-myocardial band) is also used. Serial measurements at 0, 3, and 6 hours confirm the diagnosis and estimate infarct size.
3. Chest X-Ray : Evaluates heart size, pulmonary edema (fluid in the lungs) as a sign of heart failure, and rules out other causes of chest pain such as pneumothorax or aortic dissection.
4. Echocardiography (Echo / Ultrasound) : A bedside ultrasound of the heart that visualizes wall motion abnormalities (areas of heart muscle not contracting properly), assesses ejection fraction (pumping function), detects pericardial effusion, and identifies mechanical complications such as valve rupture.
5. Coronary Angiography (Catheterization) : The definitive investigation — a thin catheter is threaded through an artery (usually radial or femoral) to the coronary arteries, where contrast dye is injected under X-ray fluoroscopy to directly visualize blockages. Performed urgently for STEMI; often combined with immediate angioplasty (PCI).
6. Additional Tests : Full blood count, renal function, lipid profile, blood glucose, coagulation studies, and thyroid function tests help assess overall risk and identify contributing factors or contraindications to therapy.
Complications of Myocardial Infarction
Depending on the size and location of the infarction, the speed of treatment, and the patient's pre-existing health, a heart attack can lead to serious short- and long-term complications.
1. Immediate & Early Complications
- Cardiac Arrhythmias — The most common early complication. Ventricular fibrillation (VF) is the leading cause of death in the first hour. Other arrhythmias include ventricular tachycardia, atrial fibrillation, and heart block. Continuous cardiac monitoring is essential.
- Cardiogenic Shock — Occurs when >40% of the left ventricular muscle is destroyed, causing the heart to be unable to maintain adequate circulation. Manifests as severe hypotension, cold extremities, and reduced urine output. Carries a mortality of 40–80% without urgent intervention.
- Acute Heart Failure & Pulmonary Edema — Weakened pumping causes blood to back up into the pulmonary circulation, flooding the lungs. Patients experience severe breathlessness and require urgent diuresis and ventilatory support.
- Mechanical Complications — Include papillary muscle rupture (causing acute mitral regurgitation), interventricular septal rupture, and free wall rupture — all surgical emergencies with high mortality.
- Pericarditis — Inflammation of the pericardial sac surrounding the heart (early pericarditis within 1–3 days, or Dressler syndrome 2–10 weeks later), causing pleuritic chest pain and fever.
2. Long-Term Complications
- Chronic Heart Failure — Persistent impairment of left ventricular function causes breathlessness, fatigue, and fluid retention, requiring lifelong management with medications and lifestyle changes.
- Ventricular Aneurysm — A thinned, bulging area of the scarred heart wall that can harbor blood clots and cause persistent ECG changes or heart failure.
- Recurrent MI & Angina — Patients with coronary artery disease remain at elevated risk for future events. Secondary prevention therapy is vital.
- Sudden Cardiac Death — Survivors of large MI with low ejection fraction are at risk of life-threatening ventricular arrhythmias; an implantable cardioverter-defibrillator (ICD) may be required.
- Psychological Impact — Depression affects 20–30% of MI survivors and independently increases the risk of recurrent events. Cardiac rehabilitation and psychological support are integral to recovery.
- Deep Vein Thrombosis (DVT) & Pulmonary Embolism — Prolonged immobility during hospital admission increases risk; prophylactic anticoagulation is standard care.
Treatment of Myocardial Infarction
Modern treatment of acute myocardial infarction focuses on three pillars: restoring blood flow as quickly as possible, protecting the heart muscle, and preventing recurrence. Treatment is divided into emergency, hospital-based, and long-term phases.
A. Emergency First Aid (Before Hospital)
- Call emergency services immediately (112 / 911 / 108 in India)
- Have the patient sit or lie down in a comfortable position; loosen tight clothing
- Administer aspirin 300–325 mg (chewed, not swallowed whole) if not allergic — inhibits platelet aggregation
- If prescribed, administer sublingual nitroglycerin for chest pain
- Be prepared to perform CPR if the patient loses consciousness and stops breathing normally
- Use an AED (Automated External Defibrillator) if available and the patient is pulseless
B. Reperfusion Therapy — Opening the Blocked Artery
- Primary PCI (Angioplasty) : Percutaneous coronary intervention — the gold standard for STEMI. A balloon catheter is used to open the blocked artery; a drug-eluting stent is placed to keep it open. Target: "door-to-balloon" time under 90 minutes.
- Thrombolysis (Clot-Busting) : Intravenous thrombolytic drugs (e.g., alteplase, tenecteplase) dissolve the clot when primary PCI is not available within 120 minutes. Most effective within 3 hours of symptom onset.
- Coronary Artery Bypass Graft (CABG) : Open-heart surgery to bypass blocked arteries using grafts from the patient's own vessels. Preferred when multiple vessels are severely blocked or PCI is not feasible.
C. Medications Used During & After MI
- Dual Antiplatelet Therapy — Aspirin + P2Y12 inhibitor (clopidogrel, ticagrelor, prasugrel) to prevent re-clotting of stent
- Anticoagulants — Heparin or LMWH given during PCI; prevents new clot formation
- Beta-Blockers — Reduce heart rate and workload; decrease mortality post-MI
- ACE Inhibitors / ARBs — Reduce cardiac remodeling and protect against heart failure
- Statins (High Intensity) — Aggressively lower LDL; stabilize plaques; reduce recurrence
- Nitroglycerin — Relieves anginal pain by dilating coronary vessels
- Morphine — Pain relief and venodilation in selected cases (use with caution)
- Oxygen — Administered if oxygen saturation <94%
D. Cardiac Rehabilitation
A structured, supervised program of exercise training, cardiovascular risk education, nutritional counseling, and psychosocial support. It is strongly recommended for all MI survivors and reduces the risk of recurrent events by 25–30%. It typically begins 4–6 weeks after the MI and continues for 3–6 months.
After discharge, patients must continue dual antiplatelet therapy (typically 12 months), lifelong aspirin, a statin, a beta-blocker, and an ACE inhibitor. Regular follow-up with a cardiologist, monitoring of blood pressure, cholesterol, and blood glucose, combined with sustained lifestyle changes, are the cornerstones of preventing a second event.
Prevention of Myocardial Infarction
The majority of first heart attacks are preventable through long-term lifestyle modifications and, where appropriate, medical therapy. Prevention is classified as primary (preventing a first event) or secondary (preventing a recurrence).
- Heart-Healthy Diet : Emphasize fruits, vegetables, whole grains, legumes, fish (omega-3s), and unsaturated fats. Minimize red meat, processed foods, trans fats, refined sugar, and excess salt. Mediterranean and DASH diets have the strongest evidence.
- Regular Physical Activity : At least 150 minutes of moderate-intensity aerobic activity (brisk walking, swimming, cycling) or 75 minutes of vigorous activity per week. Strength training 2+ days/week is also beneficial.
- Quit Smoking : Stopping smoking is the single most impactful lifestyle change. Within 1 year of quitting, MI risk drops by 50%. After 15 years, risk approaches that of a non-smoker.
- Maintain Healthy Weight : Aim for a BMI of 18.5–24.9 kg/m² and a waist circumference <94 cm (men) / <80 cm (women). Even a 5–10% reduction in body weight significantly improves cardiovascular risk factors.
- Control Blood Pressure : Target below 130/80 mmHg. Regular monitoring, low-sodium diet, exercise, stress reduction, and antihypertensive medications when needed reduce stroke and MI risk dramatically.
- Manage Cholesterol & Blood Sugar : Regular lipid screening and HbA1c testing. Use statins and anti-diabetic therapy when indicated. Tight glycemic control in diabetics reduces microvascular and macrovascular cardiovascular events.
- Stress Management : Practice mindfulness, meditation, yoga, or other stress-reduction techniques. Maintain social connections. Seek help for depression or anxiety — both are independent cardiac risk factors.
- Adequate Sleep : Sleep 7–9 hours per night. Sleep apnea — a strong risk factor for MI — should be diagnosed and treated with CPAP therapy. Poor sleep elevates inflammatory markers and blood pressure.
- Limit Alcohol : Heavy alcohol use raises blood pressure and triglycerides. If consumed, limit to no more than 1 drink/day for women, 2 for men. Current evidence does not support recommending alcohol for heart health.
- Regular Health Screening : Annual checks of BP, lipids, blood glucose, BMI, and ECG (especially after age 40 or if risk factors present). Know your numbers — hypertension and hypercholesterolemia are often silent.
- Know CPR — You Could Save a Life : Bystander CPR doubles or triples survival rates in out-of-hospital cardiac arrest. Take an accredited CPR/AED course. Hands-only CPR (100–120 compressions per minute to the center of the chest) without mouth-to-mouth is highly effective and easy to learn.
- Emergency :
 Call Emergency Services (112) India Emergency / Also try 108 (Ambulance).
Call Emergency Services (112) India Emergency / Also try 108 (Ambulance). - Do not drive yourself. Chew aspirin if not allergic. Stay calm and stay seated.
Common FAQs on Heart Attack (Myocardial Infarction)
1. What is a heart attack (myocardial infarction)?
A heart attack, or myocardial infarction (MI), occurs when blood flow through one or more coronary arteries is significantly reduced or completely blocked, depriving a portion of the heart muscle of oxygen. The most common cause is rupture of an atherosclerotic plaque followed by thrombus formation. Without prompt restoration of blood flow, myocardial tissue undergoes irreversible injury and necrosis. Heart attack is a medical emergency requiring immediate diagnosis and treatment to reduce complications, preserve cardiac function, and improve survival outcomes.
2. What are the common symptoms of a heart attack?
Common symptoms include chest pain or pressure, often described as squeezing, heaviness, or tightness, lasting more than a few minutes. The pain may radiate to the left arm, shoulder, neck, jaw, or back. Additional symptoms include shortness of breath, sweating, nausea, vomiting, dizziness, fatigue, and palpitations. Symptoms can vary among individuals, especially women, older adults, and patients with diabetes, who may present with atypical manifestations such as weakness, indigestion, or breathlessness without significant chest pain.
3. What causes a heart attack?
The primary cause of a heart attack is coronary artery disease resulting from atherosclerosis. Cholesterol-rich plaques develop within coronary arteries and may rupture, triggering clot formation that obstructs blood flow. Less common causes include coronary artery spasm, spontaneous coronary artery dissection, embolism, and severe oxygen supply-demand imbalance. Risk factors such as smoking, hypertension, diabetes mellitus, obesity, dyslipidemia, and sedentary lifestyle contribute significantly to plaque formation and progression, increasing the likelihood of myocardial infarction and related cardiovascular complications.
4. Who is at risk of developing a heart attack?
Several factors increase the risk of myocardial infarction. Non-modifiable risk factors include advancing age, male sex, and family history of premature coronary artery disease. Modifiable factors include hypertension, diabetes mellitus, dyslipidemia, smoking, obesity, physical inactivity, unhealthy diet, excessive alcohol consumption, and chronic stress. Individuals with established cardiovascular disease, chronic kidney disease, or metabolic syndrome are also at higher risk. Effective management of these risk factors can significantly reduce the incidence and severity of heart attacks.
5. How is a heart attack diagnosed?
Diagnosis of myocardial infarction is based on clinical presentation, electrocardiographic findings, and cardiac biomarkers. An electrocardiogram (ECG) helps identify ischemic changes such as ST-segment elevation, depression, or T-wave abnormalities. Elevated cardiac troponin levels confirm myocardial injury and are considered the most sensitive and specific biomarkers. Additional investigations may include echocardiography, coronary angiography, chest radiography, and laboratory tests to assess cardiac function, determine the extent of damage, and guide appropriate treatment strategies.
6. What is the difference between STEMI and NSTEMI?
ST-elevation myocardial infarction (STEMI) results from complete coronary artery occlusion and is characterized by persistent ST-segment elevation on ECG. It requires urgent reperfusion therapy to restore blood flow. Non-ST-elevation myocardial infarction (NSTEMI) usually involves partial coronary artery blockage and lacks persistent ST-segment elevation, although cardiac biomarkers remain elevated. Both conditions indicate myocardial injury and require prompt medical management. STEMI generally carries a higher risk of extensive myocardial damage, whereas NSTEMI may still lead to serious complications if untreated.
7. What should someone do during a suspected heart attack?
If a heart attack is suspected, emergency medical services should be contacted immediately. The patient should rest, remain calm, and avoid physical exertion. If not contraindicated, chewing aspirin may help inhibit platelet aggregation while awaiting medical assistance. Driving oneself to the hospital is discouraged because sudden deterioration may occur. Early recognition and rapid transport to a healthcare facility capable of performing reperfusion therapy are critical for minimizing myocardial damage and improving survival and long-term cardiovascular outcomes.
8. How is a heart attack treated?
Treatment focuses on restoring coronary blood flow and preventing further myocardial damage. Immediate therapies include antiplatelet agents, anticoagulants, nitrates, oxygen when indicated, and pain management. Reperfusion therapy is achieved through primary percutaneous coronary intervention (PCI), the preferred approach, or thrombolytic therapy when PCI is unavailable. Long-term treatment often includes statins, beta-blockers, ACE inhibitors, and lifestyle modifications. Cardiac rehabilitation programs help optimize recovery, improve functional status, and reduce the risk of recurrent cardiovascular events.
9. Can a heart attack be prevented?
Many heart attacks can be prevented through effective management of cardiovascular risk factors. Preventive measures include smoking cessation, maintaining a healthy body weight, engaging in regular physical activity, consuming a balanced diet low in saturated fats and sodium, and controlling blood pressure, cholesterol, and blood glucose levels. Routine medical evaluations are important for identifying and addressing risk factors early. Adherence to prescribed medications and healthy lifestyle practices substantially lowers the likelihood of myocardial infarction and other cardiovascular diseases.
10. What complications can occur after a heart attack?
Complications may develop depending on the size and location of the infarction. Common complications include arrhythmias, heart failure, cardiogenic shock, recurrent ischemia, ventricular septal rupture, papillary muscle dysfunction, and ventricular free wall rupture. Patients may also develop thromboembolic events, pericarditis, or chronic left ventricular dysfunction. Early diagnosis, timely reperfusion therapy, and comprehensive post-infarction care significantly reduce the risk of complications. Continuous follow-up is essential to monitor recovery and optimize long-term cardiovascular health.
11. Can a person recover completely after a heart attack?
Recovery varies according to the extent of myocardial damage, timeliness of treatment, and overall health status. Many individuals return to normal or near-normal activities after successful treatment and rehabilitation. Recovery involves medication adherence, risk-factor modification, regular follow-up, and participation in cardiac rehabilitation programs. Early intervention often limits myocardial injury and improves prognosis. Although some patients may experience permanent cardiac impairment, appropriate medical management and lifestyle changes can significantly enhance quality of life and long-term outcomes.
12. Why is early treatment important in a heart attack?
Early treatment is crucial because prolonged interruption of coronary blood flow leads to progressive myocardial necrosis. The principle “time is muscle” emphasizes that every minute of delay increases irreversible heart muscle damage. Prompt reperfusion through primary PCI or thrombolytic therapy preserves viable myocardium, reduces complications, and improves survival rates. Rapid diagnosis, emergency response, and immediate medical intervention enhance cardiac recovery and long-term prognosis. Early treatment remains one of the most important determinants of outcome in myocardial infarction.
References for Heart Attack (Myocardial Infarction)
- World Health Organization. Cardiovascular Diseases (CVDs). Geneva: World Health Organization; latest update.
- American Heart Association. Heart Disease and Stroke Statistics—Current Updates. Circulation.
- European Society of Cardiology. ESC Guidelines for the Management of Acute Coronary Syndromes. European Heart Journal.
- American College of Cardiology and American Heart Association. Guideline for the Management of Patients With Acute Myocardial Infarction.
- Braunwald's Heart Disease. Zipes DP, Libby P, Bonow RO, Mann DL, Tomaselli GF, editors. Elsevier; 2022.
- Harrison's Principles of Internal Medicine. Jameson JL, Fauci AS, Kasper DL, et al. McGraw-Hill Education; 2022.
- Davidson's Principles and Practice of Medicine. Elsevier; 2022.
- Oxford Handbook of Cardiology. Oxford University Press; 2021.