Nipah virus is a highly pathogenic zoonotic RNA virus belonging to the genus Henipavirus (family Paramyxoviridae), first identified during the 1998–1999 outbreak in Malaysia. The natural reservoir comprises fruit bats of the genus Pteropus, with transmission to humans occurring via contaminated date palm sap, direct bat exposure, or intermediate hosts such as pigs; limited human-to-human spread is documented, particularly in outbreaks in Bangladesh and India. The virus is an enveloped, negative-sense single-stranded RNA virus whose G and F glycoproteins mediate entry via ephrin-B2/B3 receptors, explaining its neurotropism and endothelial tropism. Systemic vasculitis, endothelial syncytia formation, and microinfarctions in the central nervous system are pathological hallmarks. After an incubation of 4–14 days (occasionally up to 45), patients develop acute febrile illness, headache, myalgia, vomiting, and rapidly progressive encephalitis characterized by altered sensorium, seizures, focal neurological deficits, and coma. A subset presents with severe respiratory disease including cough, dyspnea, and acute respiratory distress syndrome (ARDS). Laboratory confirmation relies on real-time RT-PCR from throat swab, cerebrospinal fluid, serum, or urine during the acute phase; IgM capture ELISA supports later diagnosis. Virus isolation requires biosafety level-4 containment. 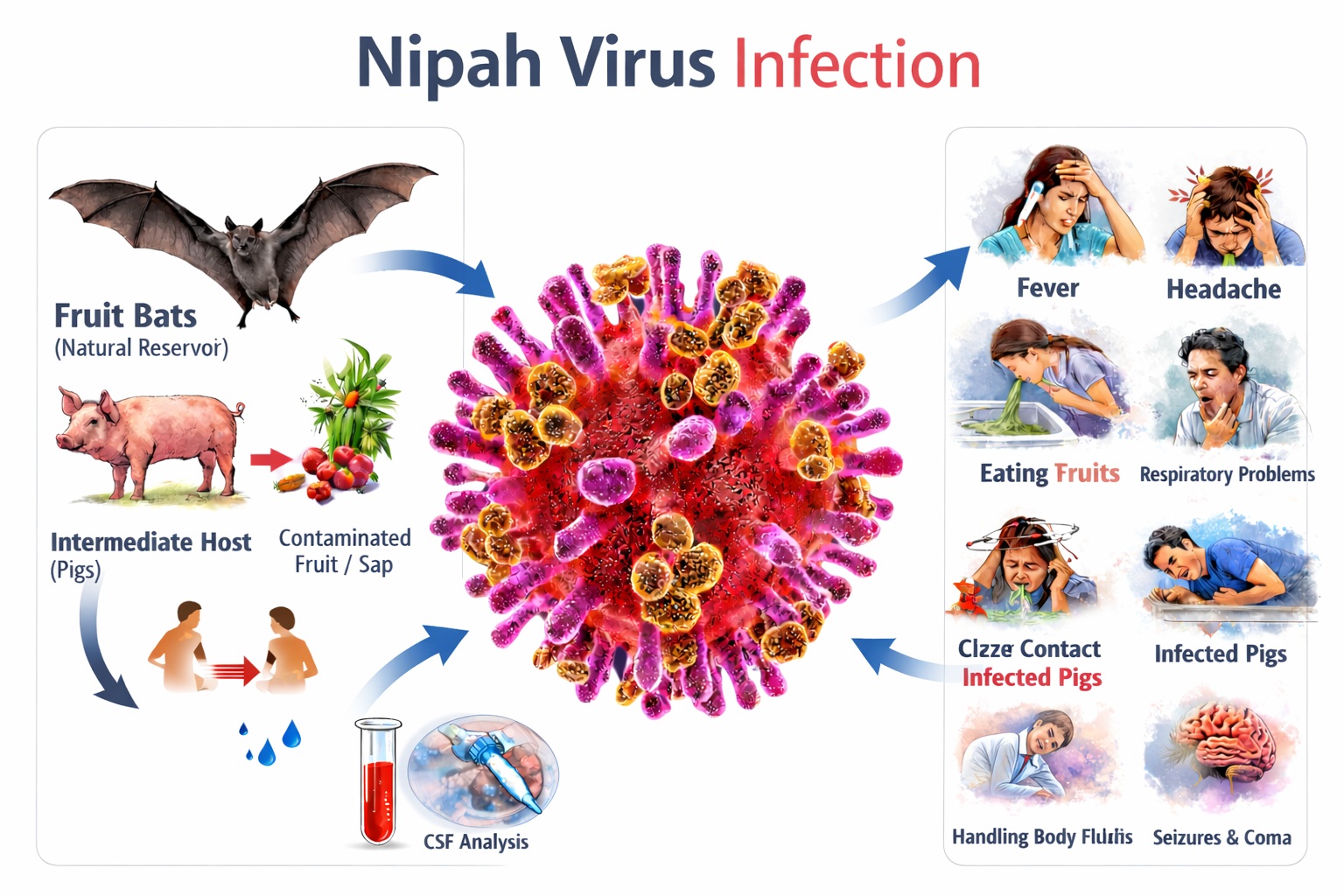
Nipah virus infection carries a high case fatality rate (40–75%, varying by outbreak and healthcare access). Major complications include refractory encephalitis, raised intracranial pressure, status epilepticus, ARDS, septic shock–like syndrome, and multiorgan dysfunction. Survivors may experience persistent neurological sequelae such as cognitive impairment, personality change, focal deficits, and, rarely, late-onset or relapsing encephalitis months to years after recovery. Pulmonary fibrosis and prolonged ventilatory dependence have been described in severe respiratory cases. There is no licensed specific antiviral therapy. Management remains largely supportive and intensive—airway protection, mechanical ventilation for ARDS, seizure control, intracranial pressure management, fluid–electrolyte balance, and prevention of secondary infections. Ribavirin has shown limited observational benefit but lacks definitive evidence. Investigational monoclonal antibodies (e.g., m102.4) and recombinant vector vaccines are under advanced development but not yet widely available. Public health measures are central to control. These include surveillance of bat reservoirs and livestock, avoidance of raw date palm sap, use of personal protective equipment in healthcare settings, rapid isolation of suspected cases, rigorous contact tracing, and community education. The World Health Organization classifies Nipah virus as a priority pathogen due to its epidemic potential, absence of licensed countermeasures, and high mortality, underscoring the importance of a One Health approach integrating human, animal, and environmental surveillance systems.
Sign and Symptoms of Nipah Virus Infection
Nipah virus infection is a severe zoonotic disease characterized by high mortality and rapid neurological deterioration. The incubation period typically ranges from 4–14 days, though extended latency up to 45 days has been documented, particularly in sporadic cases. Clinical presentation varies from asymptomatic infection to fulminant encephalitis and fatal respiratory failure. Disease severity is influenced by viral strain differences, host immune response, comorbid conditions, and access to intensive medical care. 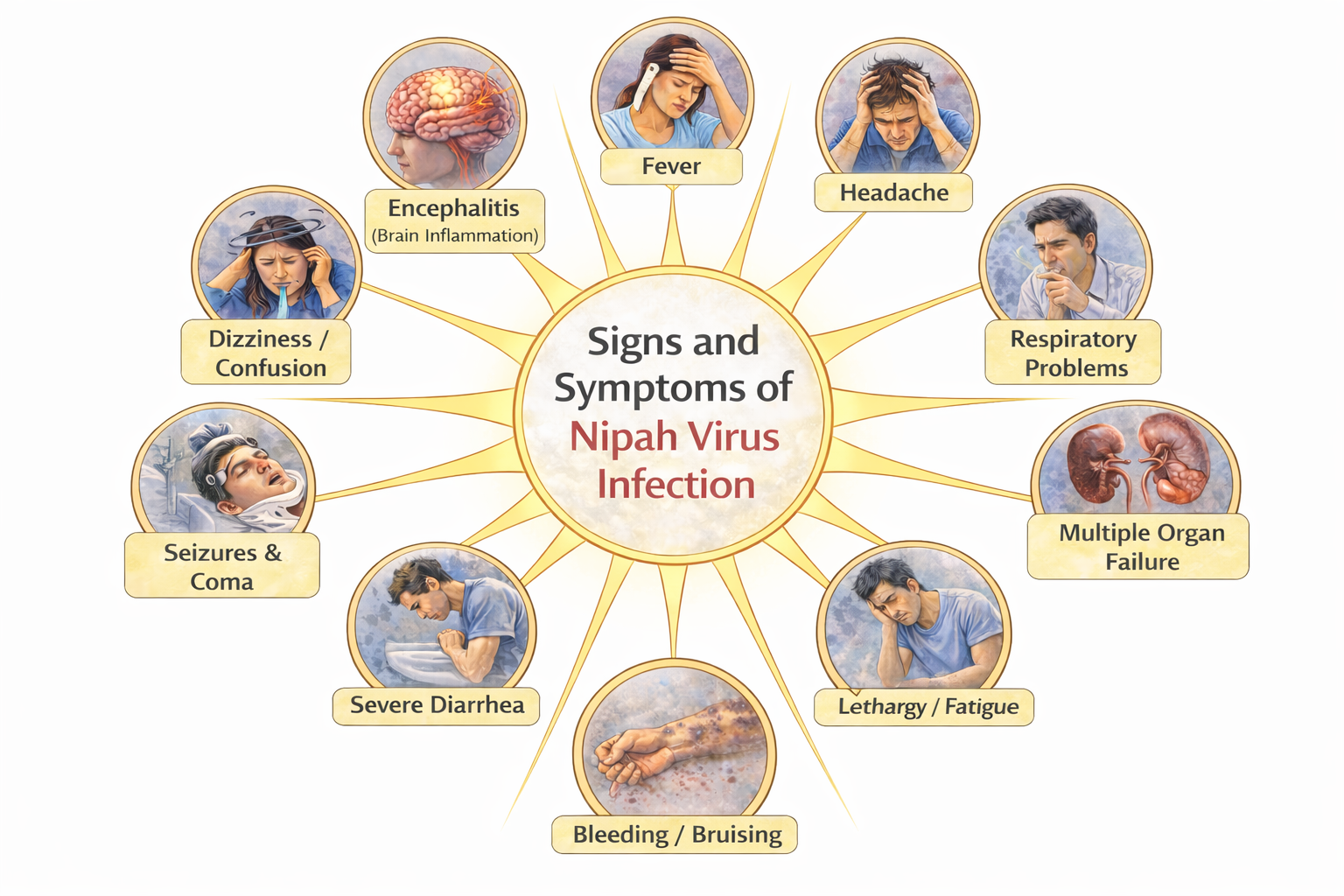
1. Early (Prodromal) Phase :
The prodromal phase resembles an acute viral febrile illness and may initially be indistinguishable from influenza or other systemic viral infections.
- High-grade fever: Usually abrupt in onset and persistent, resulting from systemic viremia and pro-inflammatory cytokine release (IL-6, TNF-α). Fever is often associated with chills and marked malaise.
- Severe headache: Diffuse and persistent, frequently retro-orbital or frontal, suggesting early meningeal irritation or central nervous system (CNS) involvement.
- Myalgia and generalized weakness: Cytokine-mediated muscle inflammation produces significant fatigue and reduced functional capacity.
- Sore throat and cough: Indicate early respiratory tract involvement and viral replication in epithelial tissues.
- Nausea, vomiting, abdominal discomfort: May occur due to systemic inflammatory response and autonomic dysfunction.
- Dizziness and lightheadedness: Could reflect early CNS effects or hemodynamic instability.
Clinical progression often occurs within 24–72 hours, transitioning to neurological or respiratory deterioration.
2. Neurological Manifestations (Acute Encephalitic Phase):
Neurological involvement represents the defining feature of severe disease and results from viral neurotropism mediated by ephrin-B2 and ephrin-B3 receptors expressed on neurons and endothelial cells.
- Altered sensorium: Progressive confusion, reduced attention span, and impaired responsiveness due to cerebral edema and inflammation.
- Drowsiness progressing to stupor: Suggests worsening encephalitis and rising intracranial pressure.
- Behavioral and personality changes: Frontal lobe dysfunction may produce irritability, agitation, or inappropriate responses.
- Seizures: Both focal and generalized seizures arise from cortical irritation, vasculitis, and microinfarctions.
- Focal neurological deficits: Hemiparesis, cranial nerve palsies, ataxia, and dysarthria may occur depending on lesion localization.
- Coma: Rapid progression to coma within 24–48 hours in severe cases, frequently associated with poor prognosis.
Histopathology demonstrates systemic vasculitis, endothelial syncytia formation, thrombosis, and neuronal necrosis, particularly affecting the brainstem and cerebral cortex.
3. Respiratory Manifestations :
Respiratory involvement is especially prominent in outbreaks reported from Bangladesh and India.
- Persistent cough and dyspnea: Reflect viral pneumonitis and inflammatory lung injury.
- Atypical pneumonia: Radiographic findings include bilateral infiltrates consistent with interstitial inflammation.
- Acute Respiratory Distress Syndrome (ARDS): Severe alveolar-capillary membrane damage leads to refractory hypoxemia, often requiring mechanical ventilation.
High viral loads in respiratory secretions significantly increase the risk of nosocomial transmission.
4. Severe and Atypical Presentations:
- Hypotension and shock-like state: A severe systemic inflammatory response may lead to peripheral vasodilation, capillary leak, and circulatory collapse, clinically resembling septic shock and requiring aggressive fluid resuscitation and vasopressor support.
- Multi-organ dysfunction: Progressive involvement of renal, hepatic, and cardiovascular systems may occur due to systemic vasculitis, endothelial injury, and impaired tissue perfusion, significantly increasing mortality risk.
- Myocarditis: Although uncommon, direct viral invasion or immune-mediated myocardial inflammation may result in reduced cardiac contractility and heart failure manifestations.
- Cardiac arrhythmias: Conduction abnormalities and rhythm disturbances may develop secondary to myocarditis, electrolyte imbalance, or systemic inflammatory stress.
- Laboratory abnormalities: Thrombocytopenia, elevated hepatic transaminases, leukopenia or leukocytosis, metabolic acidosis, and impaired renal parameters may be observed, reflecting systemic involvement and disease severity.
5. Late and Long-Term Sequelae :
- Cognitive impairment: Survivors may experience persistent deficits in attention, executive function, and processing speed due to residual neuronal damage.
- Memory disturbances: Short-term and long-term memory impairment may occur, affecting daily functioning and occupational performance.
- Personality and behavioral changes: Frontal lobe involvement can lead to irritability, mood instability, depression, or altered social behavior.
- Persistent fatigue: Chronic post-viral fatigue may significantly limit physical endurance and quality of life.
- Motor dysfunction: Residual weakness, coordination problems, or movement abnormalities may persist due to focal neurological injury.
- Relapsing or late-onset encephalitis: Rare cases develop renewed neurological symptoms months to years after recovery, possibly associated with viral persistence in central nervous system tissues or delayed immune-mediated mechanisms.
Nipah virus infection is a severe zoonotic disease, presenting initially with fever, headache, and myalgia, rapidly progressing to encephalitis, seizures, coma, or acute respiratory distress. Multi-organ dysfunction may occur. Survivors risk persistent neurological deficits. Case fatality ranges 40–75%, requiring intensive supportive management and strict infection control. Early diagnosis, strict infection prevention measures, and aggressive supportive care remain critical determinants of survival and long-term neurological outcome. Nipah virus infection typically begins as an acute febrile illness characterized by high-grade fever, severe headache, myalgia, malaise, and sore throat. As viral replication progresses and systemic inflammation develops, patients may develop nausea, vomiting, dizziness, and respiratory symptoms such as cough and shortness of breath due to viral pneumonitis. The hallmark of severe disease is rapid neurological deterioration caused by viral encephalitis. Patients may develop confusion, altered mental status, seizures, focal neurological deficits, and reduced level of consciousness that can progress to coma within 24–48 hours. Some patients also develop autonomic instability, abnormal reflexes, and brainstem dysfunction leading to respiratory failure. The rapid progression from mild symptoms to severe neurological compromise is a distinguishing clinical feature and requires immediate medical attention and isolation.
Risk Factors of Nipah virus Infection
Nipah virus infection is closely associated with ecological interfaces between wildlife, domestic animals, and humans. Transmission risk is determined by environmental exposure, occupational contact, healthcare practices, and host susceptibility. Outbreak patterns in Bangladesh, India, and Malaysia illustrate the multifactorial nature of risk determinants. 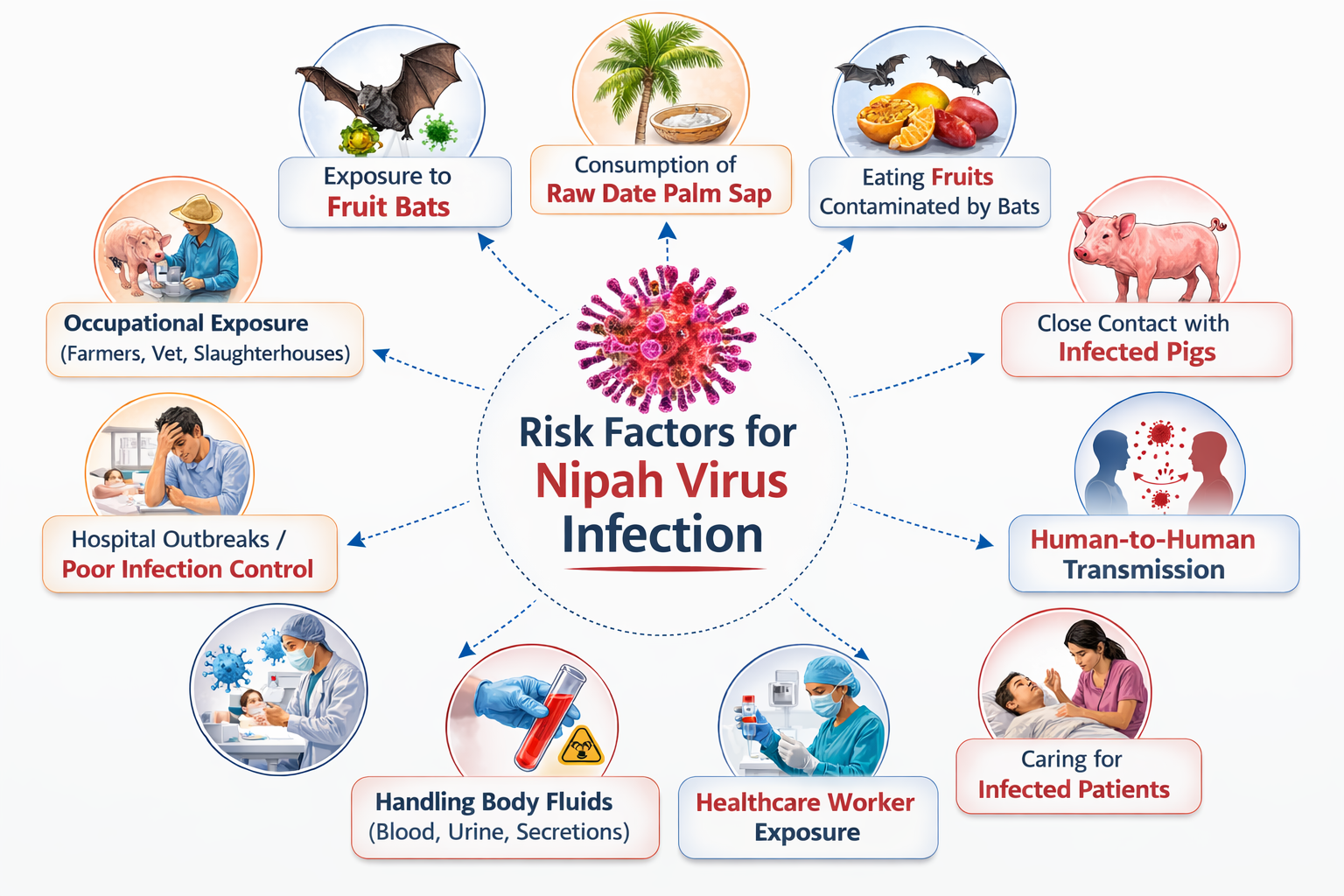
-
Animal and Environmental Exposure
- Contact with fruit bats (Pteropus species): Fruit bats are the natural reservoirs of Nipah virus. Direct handling of bats, exposure to bat excreta, or contact with fruits partially eaten by bats facilitates zoonotic spillover through mucosal or cutaneous exposure.
- Consumption of raw date palm sap: Fresh date palm sap collected in open containers may be contaminated by bat saliva or urine during nocturnal feeding. Ingestion of unboiled sap represents a major primary transmission route in South Asian outbreaks.
- Exposure to infected livestock (particularly pigs): During the Malaysian outbreak, pigs acted as amplification hosts. Farmers, abattoir workers, and veterinarians exposed to respiratory secretions and aerosols from infected pigs experienced high infection rates.
- Deforestation and habitat encroachment: Agricultural expansion and urbanization disrupt bat habitats, increasing bat–human proximity and viral spillover risk due to altered feeding and roosting behavior.
- Seasonal factors: Sap-harvesting seasons and bat breeding cycles may influence viral shedding and increase seasonal clustering of cases.
-
Human-to-Human Transmission Risks
- Close physical contact with infected patients: Direct exposure to saliva, respiratory droplets, urine, or other body fluids significantly increases infection risk, particularly during advanced respiratory disease.
- Healthcare-associated transmission: Inadequate infection prevention and control (IPC) measures, absence of appropriate personal protective equipment (PPE), and aerosol-generating procedures (intubation, suctioning) enhance nosocomial spread.
- Caregiving practices: Family members providing prolonged bedside care without protective barriers face high exposure risk due to sustained close contact.
- Delayed isolation: Late recognition of cases increases secondary transmission within hospitals and communities.
-
Host-Related Risk Factors
- Immunocompromised individuals: Patients with weakened immunity (e.g., chronic illness, malnutrition) may be more susceptible to infection and severe disease progression.
- Comorbid medical conditions: Diabetes mellitus, chronic kidney disease, cardiovascular disorders, and chronic respiratory diseases may worsen clinical outcomes and increase mortality risk.
- Extremes of age: Elderly individuals are more likely to develop severe encephalitis and respiratory complications due to reduced physiological reserve.
- Poor nutritional status: Malnutrition may impair immune response, increasing susceptibility and severity.
-
Occupational Risk Factors
- Pig farmers and animal handlers: Repeated close exposure to infected animals, contaminated fomites, and respiratory aerosols increases occupational hazard.
- Healthcare workers: Physicians, nurses, laboratory personnel, and support staff are at elevated risk without strict adherence to standard and droplet precautions.
- Laboratory personnel: Handling clinical specimens without appropriate biosafety level-3/4 precautions may result in accidental exposure.
- Sap collectors and agricultural workers: Occupational exposure during sap harvesting or fruit collection increases zoonotic risk.
-
Community and Socioeconomic Determinants
- Overcrowding: Dense living conditions facilitate rapid human-to-human transmission during outbreaks.
- Limited healthcare access: Delayed diagnosis, inadequate isolation facilities, and lack of intensive care infrastructure increase transmission and mortality.
- Low public awareness: Cultural practices such as consumption of raw palm sap and traditional caregiving without protective measures enhance exposure risk.
- Weak surveillance systems: Insufficient disease monitoring may delay outbreak detection and containment.
Nipah virus infection risk reflects a complex interplay between environmental exposure, occupational hazards, healthcare practices, and host vulnerability. Effective mitigation requires an integrated One Health strategy, emphasizing wildlife surveillance, community education, strict infection control, and strengthened public health infrastructure. Risk factors for Nipah virus infection are primarily related to zoonotic exposure and close human contact with infected individuals. The natural reservoir of the virus is fruit bats of the genus Pteropus, and transmission often occurs through consumption of food contaminated with bat saliva, urine, or partially eaten fruits. Drinking raw date palm sap contaminated by bats has been a major transmission route in outbreaks in South Asia. Occupational exposure among farmers, animal handlers, veterinarians, and slaughterhouse workers increases the likelihood of infection through contact with infected animals such as pigs or bats. Human-to-human transmission can occur in healthcare settings through close contact with respiratory secretions, body fluids, or contaminated surfaces, particularly when infection-control measures are inadequate. Living in endemic regions, participation in caregiving for infected patients, and delayed recognition of the disease during outbreaks significantly increase the risk of transmission and infection.
Diagnosis of Nipah virus Infection
Diagnosis of Nipah virus infection requires a meticulous and multidisciplinary approach integrating clinical examination, epidemiological linkage, laboratory confirmation, imaging findings, and dynamic interpretation of disease progression. Because of its rapid neurological deterioration and high mortality, early bedside suspicion is critical even before laboratory confirmation. All suspected cases must be managed with strict infection prevention precautions. 
1. Clinical Examination
A. General Physical Examination
- Fever Pattern: Fever is typically high-grade (>38.5–39°C), continuous or remittent, and often refractory to routine antipyretics. It reflects systemic viral replication and cytokine storm. Persistent fever beyond 48 hours with neurological signs increases suspicion of viral encephalitis rather than simple febrile illness.
- Level of Consciousness (Glasgow Coma Scale – GCS): Early stages may show subtle cognitive slowing or irritability (GCS 14–15). Rapid decline to confusion (GCS 12–13), stupor (GCS 9–11), or coma (GCS ≤8) indicates severe cerebral inflammation, edema, or brainstem involvement. Serial GCS monitoring is crucial for prognostic assessment.
- Hemodynamic Parameters:
- Tachycardia may result from fever, dehydration, or systemic inflammatory response syndrome (SIRS).
- Hypotension suggests capillary leak, systemic vasodilation, or evolving septic shock–like state.
- Poor peripheral perfusion (cold extremities, delayed capillary refill) indicates circulatory compromise.
- Respiratory Rate and Oxygenation: Tachypnea (>24/min in adults) and declining oxygen saturation (<94% on room air) suggest evolving pneumonitis or acute lung injury.
A febrile patient with rapid neurological decline, unstable vitals, and hypoxemia in an endemic setting strongly suggests Nipah virus infection requiring urgent isolation.
B. Detailed Neurological Examination
- Mental Status and Higher Functions: Impaired attention, disorientation, memory deficits, agitation, or apathy reflect cortical and limbic system involvement. Early personality changes may precede overt coma.
- Cranial Nerve Examination:
- Facial asymmetry suggests VII nerve involvement.
- Dysarthria and dysphagia indicate bulbar palsy.
- Ophthalmoplegia or nystagmus may indicate brainstem pathology.
- Motor Examination:
- Increased tone (spasticity) suggests upper motor neuron lesion.
- Hemiparesis or quadriparesis may occur due to focal vasculitic infarctions.
- Positive Babinski sign indicates corticospinal tract involvement.
- Sensory Examination: May show subtle deficits due to focal cortical involvement.
- Cerebellar Function: Ataxia, intention tremor, or impaired coordination reflect cerebellar or brainstem lesions.
- Seizure Assessment: Seizures may be focal (suggesting localized cortical damage) or generalized. Status epilepticus is associated with poor prognosis.
Multifocal deficits with rapid progression strongly indicate encephalitis with vasculitic microinfarctions, characteristic of Nipah neuropathology.
C. Respiratory System Examination
- Inspection: Nasal flaring, intercostal retractions, and use of accessory muscles indicate respiratory distress.
- Palpation: Reduced chest expansion may suggest diffuse alveolar involvement.
- Percussion: May reveal dullness in consolidated lung areas.
- Auscultation: Fine or coarse crackles bilaterally suggest interstitial pneumonitis; decreased breath sounds may indicate severe alveolar damage.
- Oxygenation Status: Pulse oximetry and arterial blood gas analysis may show hypoxemia (PaO₂ <60 mmHg) and respiratory alkalosis progressing to metabolic acidosis in severe ARDS.
Severe respiratory findings correlate with high viral shedding and increased mortality risk.
2. Laboratory Diagnosis and Interpretation
A. Molecular Testing
- Real-Time RT-PCR (Gold Standard): Detects viral RNA in throat swab, nasal swab, CSF, serum, urine, or endotracheal aspirates.
- Highest sensitivity during early acute phase (first 3–10 days).
- Cycle threshold (Ct) values inversely correlate with viral load; lower Ct indicates higher viral burden.
- Repeat testing may be necessary if early result is negative but suspicion remains high.
- Whole Genome Sequencing: Useful for strain identification, phylogenetic mapping, mutation tracking, and outbreak source tracing.
Positive RT-PCR confirms active infection; high viral load may correlate with severe disease.
B. Serological Testing
- IgM ELISA: Detectable after 3–5 days; confirms recent infection.
- IgG ELISA: Appears later; indicates past exposure or recovery.
- Neutralization Assays: Confirm antibody specificity; performed under high-containment conditions.
IgM positivity with compatible symptoms supports diagnosis, particularly in late presenters.
C. Hematological and Biochemical Parameters
- Complete Blood Count: Thrombocytopenia due to endothelial injury and consumption. Leukopenia suggests viral suppression; leukocytosis may reflect secondary infection.
- Liver Function Tests: Elevated AST/ALT reflect hepatic inflammation secondary to systemic infection.
- Renal Function Tests: Elevated creatinine indicates renal hypoperfusion or multiorgan dysfunction.
- Electrolytes: Hyponatremia may occur due to SIADH or severe illness.
- Inflammatory Markers: Elevated CRP and procalcitonin may reflect systemic inflammation.
- Arterial Blood Gas (ABG): Hypoxemia, respiratory alkalosis (early), metabolic acidosis (late) indicate worsening respiratory and systemic compromise.
D. Cerebrospinal Fluid (CSF) Examination
- Mild to moderate lymphocytic pleocytosis
- Elevated protein levels
- Normal or mildly decreased glucose
Typical viral encephalitis pattern; absence of neutrophilic predominance helps differentiate from bacterial meningitis.
3. Radiological and Ancillary Investigations
- MRI Brain (Preferred Imaging): T2/FLAIR hyperintense lesions in subcortical white matter, corpus callosum, brainstem, and basal ganglia. These represent microinfarctions from vasculitis and endothelial damage. Diffusion-weighted imaging may show restricted diffusion.
- CT Brain: May be normal in early stages; less sensitive than MRI.
- Chest X-ray / CT Thorax: Bilateral ground-glass opacities or diffuse alveolar infiltrates suggest viral pneumonitis or ARDS.
- Electroencephalography (EEG): Diffuse slowing consistent with encephalopathy; periodic discharges may indicate severe cortical dysfunction.
Diagnosis of Nipah virus infection is confirmed by RT-PCR positivity, but early clinical suspicion based on rapid neurological decline, respiratory compromise, epidemiological exposure, and supportive laboratory and imaging findings is critical. Serial clinical assessment, monitoring of GCS, oxygenation status, and laboratory parameters help assess disease progression and prognosis. Immediate isolation, infection control measures, and supportive intensive care are essential to limit transmission and improve survival. Diagnosis of Nipah virus infection requires integration of clinical suspicion, epidemiological exposure history, and laboratory confirmation. Because early symptoms resemble other febrile illnesses or viral encephalitis, physicians must maintain a high index of suspicion in patients presenting with acute neurological symptoms or severe respiratory illness in endemic areas. The definitive diagnosis is made through molecular detection of viral RNA using real-time reverse transcriptase polymerase chain reaction (RT-PCR) performed on throat swabs, nasal swabs, cerebrospinal fluid, blood, urine, or respiratory samples. Serological testing such as IgM and IgG ELISA can identify recent or past infection, particularly in later stages of illness. Cerebrospinal fluid examination may show findings consistent with viral encephalitis, including lymphocytic pleocytosis and elevated protein. Neuroimaging such as MRI may reveal multiple small lesions in the brain caused by vasculitic microinfarctions. Early laboratory confirmation combined with clinical assessment is essential for prompt isolation and outbreak control.
Complications of Nipah virus Infection
Complications of Nipah virus infection develop as a consequence of widespread viral replication, endothelial cell infection, immune-mediated inflammatory responses, and systemic vasculitis affecting multiple organ systems. The virus exhibits a particular affinity for neuronal tissues, vascular endothelium, and respiratory epithelium, resulting in pathological processes such as necrotizing vasculitis, endothelial syncytia formation, microvascular thrombosis, and parenchymal necrosis. These pathological alterations impair microcirculation and disrupt normal tissue perfusion, eventually leading to organ dysfunction. Clinically, complications may appear during the acute viremic phase, during the encephalitic stage of illness, or during recovery as delayed neurological sequelae. In severe cases, multiple organs may become involved simultaneously, producing life-threatening systemic disease. Careful monitoring of neurological status, respiratory function, cardiovascular stability, and biochemical parameters is therefore essential for early recognition and effective management of complications. 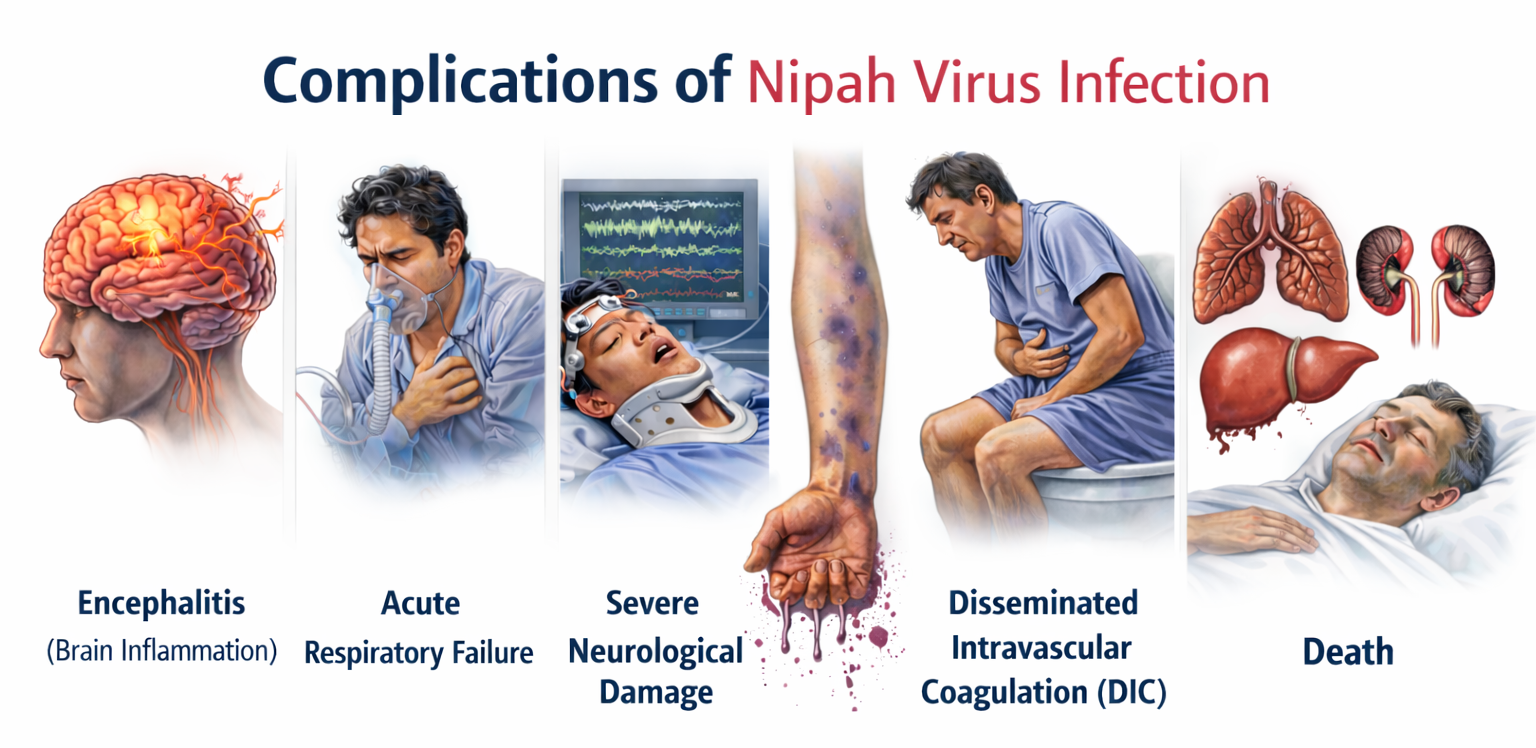
A. Neurological Complications
1. Acute Viral Encephalitis
Acute viral encephalitis is the most characteristic and severe neurological complication of Nipah virus infection. The virus enters the central nervous system through hematogenous dissemination and infects cerebral endothelial cells and neurons. This leads to widespread inflammation of brain tissue, vascular injury, and formation of microvascular thrombi that impair cerebral blood flow. As a result, neuronal damage occurs in multiple regions of the brain, producing neurological symptoms such as severe headache, persistent fever, confusion, agitation, and progressive decline in consciousness. Patients may rapidly deteriorate from mild cognitive impairment to stupor or deep coma within a short period, reflecting severe encephalitic involvement.
Histopathologically, Nipah virus encephalitis is characterized by necrotizing vasculitis, endothelial syncytia formation, and multiple microinfarctions within the brain parenchyma. These lesions disrupt neuronal signaling pathways and contribute to widespread neurological deficits. Without prompt supportive care and close neurological monitoring, severe encephalitis may progress to irreversible brain injury or death.
2. Cerebral Edema and Raised Intracranial Pressure
Cerebral edema frequently accompanies encephalitis in Nipah virus infection and results from inflammatory injury to cerebral blood vessels. Cytokine-mediated increases in vascular permeability allow plasma and inflammatory cells to accumulate within brain tissues, producing swelling of the cerebral parenchyma. Because the cranial cavity is rigid and cannot expand, this swelling leads to elevated intracranial pressure. Clinically, patients may develop severe persistent headache, nausea, vomiting, photophobia, and progressive decline in consciousness.
As intracranial pressure continues to rise, compression of vital brain structures may occur. Fundoscopic examination may reveal papilledema, and neurological examination may show abnormal pupillary reflexes or reduced responsiveness. In advanced cases, increased intracranial pressure may lead to brain herniation syndromes such as uncal or tonsillar herniation, which can disrupt brainstem function and cause sudden respiratory or cardiovascular collapse.
3. Seizure Disorders
Seizures are commonly observed in patients with Nipah virus encephalitis and occur as a result of cortical irritation, neuronal injury, and microvascular ischemia within the brain. Seizures may present as focal motor seizures originating from specific cortical regions or as generalized tonic–clonic seizures reflecting widespread neuronal involvement. In severe cases, patients may develop status epilepticus, a life-threatening condition characterized by prolonged or repeated seizures without recovery of consciousness.
Seizure activity significantly increases metabolic demand in the brain and may exacerbate neuronal injury by causing cerebral hypoxia and metabolic disturbances. Recurrent seizures may also contribute to increased intracranial pressure and further deterioration of neurological function. Effective seizure management and continuous neurological monitoring are therefore essential in the clinical care of patients with Nipah virus infection.
4. Brainstem Dysfunction
In advanced stages of the disease, the virus may involve the brainstem, which contains critical centers responsible for controlling respiration, cardiovascular function, and cranial nerve activity. Viral infection and inflammation within brainstem nuclei can disrupt autonomic regulation and produce a variety of neurological deficits. Patients may experience dysphagia, dysarthria, impaired gag reflex, cranial nerve palsies, abnormal eye movements, and facial weakness.
Brainstem dysfunction may also interfere with central respiratory control, leading to irregular breathing patterns or respiratory arrest. Because the brainstem plays a vital role in maintaining essential life functions, its involvement is considered a poor prognostic indicator. Patients with brainstem involvement often require intensive care support due to the risk of respiratory failure and cardiovascular instability.
5. Persistent Neurological Sequelae and Relapsing Encephalitis
Among survivors of acute Nipah virus infection, long-term neurological complications are relatively common. These sequelae arise from irreversible neuronal injury, gliosis, and structural damage to brain tissues caused by the acute encephalitic process. Patients may experience cognitive impairment, memory deficits, reduced concentration, personality changes, mood disturbances, and chronic fatigue. Motor abnormalities such as tremors, weakness, or impaired coordination may also occur depending on the regions of the brain affected.
In rare cases, individuals who initially recover from Nipah virus infection may develop relapsing or late-onset encephalitis months or even years after the initial illness. This delayed complication is believed to result from persistent viral reservoirs within central nervous system tissues or delayed immune-mediated inflammatory responses. Clinically, relapsing encephalitis may present with recurrent seizures, behavioral changes, and progressive neurological deterioration.
B. Respiratory Complications
1. Viral Pneumonitis
Viral pneumonitis is a common respiratory complication of Nipah virus infection and results from direct infection of respiratory epithelial cells lining the bronchioles and alveoli. Viral replication within these cells leads to diffuse inflammation of pulmonary tissues, destruction of epithelial cells, and accumulation of inflammatory exudates within alveoli. This process impairs normal gas exchange and results in respiratory symptoms such as persistent cough, chest discomfort, dyspnea, and tachypnea.
Radiological imaging of the chest often demonstrates bilateral infiltrates or ground-glass opacities reflecting diffuse interstitial inflammation. In severe cases, progressive pulmonary involvement may lead to worsening hypoxemia and respiratory distress, requiring oxygen therapy or ventilatory support.
2. Acute Respiratory Distress Syndrome (ARDS)
Acute respiratory distress syndrome represents one of the most severe pulmonary complications associated with Nipah virus infection. It develops when inflammatory injury to the alveolar-capillary membrane increases vascular permeability, allowing protein-rich fluid to accumulate within alveoli. This accumulation severely impairs oxygen diffusion and reduces lung compliance.
Clinically, patients with ARDS present with severe shortness of breath, rapid breathing, cyanosis, and refractory hypoxemia that does not improve with conventional oxygen therapy. Mechanical ventilation is often required to maintain adequate oxygenation. ARDS is associated with high mortality due to the severity of pulmonary damage and the difficulty of restoring effective gas exchange.
3. Respiratory Failure
Respiratory failure occurs when extensive lung injury prevents the respiratory system from maintaining adequate oxygenation and carbon dioxide elimination. Progressive alveolar damage reduces pulmonary compliance and increases the work of breathing, eventually causing respiratory muscle fatigue. Patients may develop severe hypoxemia, tachypnea, cyanosis, and altered mental status due to insufficient oxygen supply to the brain.
Respiratory failure may also be exacerbated by brainstem involvement, which disrupts central respiratory control. Patients with severe respiratory failure often require intensive care management, including mechanical ventilation and continuous monitoring of arterial blood gases.
4. Secondary Respiratory Infections
Patients with severe Nipah virus infection may become susceptible to secondary bacterial infections of the respiratory tract. Prolonged hospitalization, mechanical ventilation, and immune dysfunction increase the risk of developing bacterial pneumonia or ventilator-associated infections. These secondary infections may worsen respiratory function and prolong recovery.
Clinically, secondary infections may present with new fever spikes, purulent sputum, worsening respiratory distress, and elevated inflammatory markers. Early identification and appropriate antimicrobial therapy are essential to prevent further complications.
C. Cardiovascular Complications
1. Myocarditis
Myocarditis refers to inflammation of the heart muscle that may occur as a complication of severe viral infection. In Nipah virus infection, myocardial injury may occur due to systemic inflammatory responses and immune-mediated damage to cardiac tissues. Inflammation of cardiac muscle fibers can impair contractility and disrupt normal electrical conduction.
Patients with myocarditis may experience palpitations, chest discomfort, fatigue, and arrhythmias. In severe cases, myocardial dysfunction may lead to reduced cardiac output and progression to heart failure. Continuous cardiac monitoring is therefore important in critically ill patients.
2. Hypotensive Shock
Systemic inflammatory responses during severe Nipah virus infection may produce profound vasodilation and increased vascular permeability. This leads to leakage of plasma from blood vessels and reduction of effective circulating blood volume, resulting in hypotension. Clinically, patients may present with tachycardia, low blood pressure, cold extremities, and reduced urine output.
Persistent hypotension despite adequate fluid resuscitation may indicate progression to shock. If untreated, this condition can lead to impaired perfusion of vital organs and development of multiorgan failure.
3. Cardiac Arrhythmias
Cardiac arrhythmias may occur due to myocardial inflammation, electrolyte imbalance, or systemic metabolic disturbances. Abnormal heart rhythms may include tachycardia, bradycardia, or irregular cardiac conduction patterns detectable on electrocardiography.
Severe arrhythmias may compromise cardiac output and worsen hemodynamic instability. Continuous cardiac monitoring is therefore recommended for patients with severe infection, especially those admitted to intensive care units.
D. Renal Complications
1. Acute Kidney Injury
Acute kidney injury may occur due to reduced renal perfusion, systemic inflammation, and microvascular thrombosis affecting renal circulation. These processes impair glomerular filtration and lead to accumulation of metabolic waste products in the bloodstream. Patients may develop reduced urine output, fluid retention, and elevated serum creatinine levels.
If renal dysfunction progresses, electrolyte imbalance and metabolic acidosis may occur, further complicating the patient’s clinical condition. Severe cases may require renal replacement therapy such as dialysis to maintain metabolic stability.
2. Electrolyte Imbalance
Renal dysfunction and systemic illness may lead to disturbances in electrolyte balance. Hyponatremia is commonly observed and may result from inappropriate antidiuretic hormone secretion or impaired renal function. Other electrolyte abnormalities such as hyperkalemia or metabolic acidosis may also occur.
These metabolic disturbances may worsen neurological symptoms, increase the risk of cardiac arrhythmias, and complicate overall patient management. Regular monitoring of serum electrolytes is therefore essential.
E. Hematological Complications
1. Thrombocytopenia
Thrombocytopenia is frequently observed in severe Nipah virus infection due to endothelial injury, platelet consumption, and immune-mediated destruction of platelets. Reduced platelet counts increase the risk of bleeding and may manifest clinically as petechiae, easy bruising, or mucosal bleeding.
Persistent thrombocytopenia may also reflect severe systemic inflammation and endothelial damage. Monitoring platelet levels is important for assessing disease severity and guiding supportive management.
2. Disseminated Intravascular Coagulation
Disseminated intravascular coagulation is a severe complication characterized by widespread activation of coagulation pathways. Excessive clot formation within the microvasculature consumes clotting factors and platelets, leading to both thrombosis and bleeding tendencies.
Laboratory findings may include prolonged coagulation times, reduced fibrinogen levels, elevated D-dimer concentrations, and thrombocytopenia. Clinically, patients may develop bleeding from mucosal surfaces, internal hemorrhage, or organ ischemia due to microvascular thrombosis.
F. Systemic Complication
Multiorgan Dysfunction Syndrome (MODS)
Multiorgan dysfunction syndrome represents the final and most severe complication of Nipah virus infection. It occurs when systemic inflammation, endothelial injury, and impaired microcirculation lead to progressive failure of multiple organ systems including the brain, lungs, heart, liver, and kidneys. Patients with MODS may present with severe hypotension, respiratory failure, metabolic acidosis, reduced urine output, and progressive decline in consciousness.
This condition requires intensive care management involving ventilatory support, hemodynamic stabilization, and correction of metabolic abnormalities. Despite aggressive treatment, MODS is associated with a high mortality rate and represents the terminal pathway in many fatal cases of Nipah virus infection.
Nipah virus infection can lead to severe complications due to widespread endothelial damage, systemic vasculitis, and multiorgan involvement. The most serious complication is acute viral encephalitis, which results in cerebral edema, seizures, coma, and potentially permanent neurological damage in survivors. Respiratory complications such as viral pneumonitis and acute respiratory distress syndrome may lead to severe hypoxemia and respiratory failure requiring mechanical ventilation. Cardiovascular complications including hypotension, shock, and myocarditis may occur due to systemic inflammatory response and vascular injury. Multiorgan dysfunction involving the liver and kidneys can develop in advanced disease. Some survivors experience long-term neurological sequelae such as persistent seizures, personality changes, or cognitive impairment. Relapsing or late-onset encephalitis has also been reported months or years after apparent recovery, highlighting the chronic neurological risk associated with this infection.
Treatment of Nipah virus Infection
The treatment of Nipah virus infection is largely supportive and intensive-care oriented because there is currently no universally approved curative antiviral therapy. Management focuses on early diagnosis, strict infection control, stabilization of vital functions, treatment of neurological and respiratory complications, and prevention of multiorgan failure. Due to the high mortality rate and the potential for person-to-person transmission, patients must be managed in specialized isolation units with multidisciplinary medical care. The following major treatment components are considered essential in both academic understanding and clinical practice. 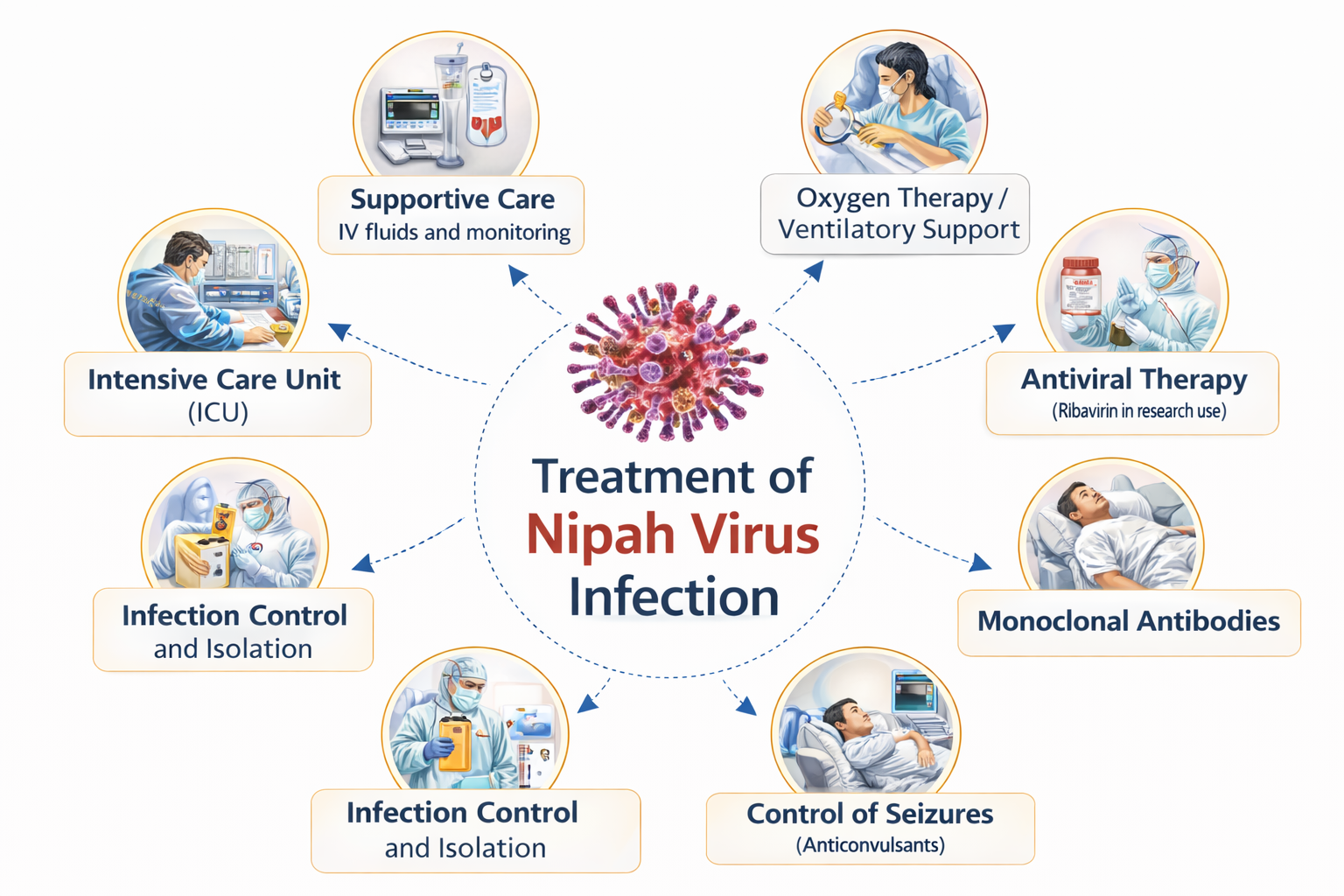
A. Infection Control and Isolation Measures
1. Patient Isolation
Patients suspected or confirmed to have Nipah virus infection must be immediately isolated in specialized hospital units to prevent transmission to healthcare workers and other patients. Ideally, patients should be admitted to negative-pressure isolation rooms where airflow systems reduce the spread of infectious droplets. Isolation minimizes exposure to respiratory secretions, saliva, urine, and other bodily fluids that may contain the virus.
From a clinical perspective, early isolation is essential because Nipah virus has demonstrated significant nosocomial transmission in previous outbreaks. Delayed isolation can lead to rapid spread within hospitals, affecting healthcare workers and family members. Therefore, strict patient isolation protocols play a critical role in outbreak containment and protection of medical staff.
2. Use of Personal Protective Equipment (PPE)
Healthcare personnel managing infected patients must use complete personal protective equipment including N95 respirators, gloves, gowns, eye protection, and face shields. These protective barriers reduce the risk of viral transmission through droplets, aerosols, or contact with contaminated surfaces. Proper training in donning and removing PPE is equally important to prevent accidental exposure.
In clinical practice, failure to follow PPE protocols has been associated with healthcare-associated outbreaks. Continuous monitoring of infection control practices, supervision of healthcare staff, and adequate availability of protective equipment are necessary to maintain safety in healthcare settings.
3. Environmental Disinfection and Waste Management
Contaminated surfaces, medical equipment, and hospital environments must be regularly disinfected using appropriate virucidal agents such as sodium hypochlorite solutions. Medical waste generated during patient care should be disposed of according to strict biomedical waste management protocols to prevent environmental contamination.
Effective environmental sanitation helps reduce viral persistence in healthcare settings. Proper waste management also prevents indirect transmission of the virus through contaminated materials, which is particularly important during large outbreaks.
B. Supportive Clinical Management
1. Fluid and Electrolyte Management
Patients with Nipah virus infection frequently develop dehydration due to fever, vomiting, reduced oral intake, and systemic illness. Intravenous fluid therapy is therefore essential to maintain adequate hydration and ensure proper organ perfusion. Electrolyte levels such as sodium, potassium, and chloride must be closely monitored because imbalances can worsen neurological and cardiovascular complications.
Careful fluid management is important because excessive fluid administration may aggravate pulmonary complications such as acute respiratory distress syndrome. Physicians must therefore balance fluid resuscitation with the patient’s respiratory status to prevent fluid overload.
2. Fever and Symptom Control
High fever is one of the most common manifestations of Nipah virus infection and contributes to metabolic stress, dehydration, and patient discomfort. Antipyretic medications such as paracetamol are commonly used to reduce fever and improve patient comfort. Other symptomatic treatments may include antiemetics for nausea and vomiting and analgesics for headache and muscle pain.
Symptom control is clinically important because it improves patient tolerance to illness and reduces metabolic demands on the body. Proper symptomatic treatment also facilitates monitoring of disease progression by preventing confounding symptoms.
3. Nutritional Support
Severely ill patients often experience reduced appetite, swallowing difficulties, or altered consciousness that limits oral intake. Nutritional support may therefore be provided through enteral feeding via nasogastric tubes or parenteral nutrition when necessary. Adequate nutrition is essential for immune function, tissue repair, and overall recovery.
Malnutrition during severe infections can worsen immune suppression and delay recovery. For this reason, maintaining adequate caloric and protein intake is an important component of supportive care.
C. Antiviral and Investigational Therapies
1. Ribavirin Therapy
Ribavirin is a broad-spectrum antiviral drug that has been used experimentally during several Nipah virus outbreaks. The drug acts by interfering with viral RNA synthesis and replication, potentially reducing viral load in infected patients. Some observational studies conducted during outbreaks suggested that ribavirin may reduce mortality rates.
However, clinical evidence regarding the effectiveness of ribavirin remains limited and inconsistent. While it may be used in certain clinical settings as part of experimental or compassionate therapy, it is not considered a definitive treatment. Ongoing research continues to evaluate its therapeutic potential.
2. Monoclonal Antibody Therapy
Recent advances in virology have led to the development of monoclonal antibodies targeting Nipah virus surface glycoproteins. One of the most promising experimental therapies is the monoclonal antibody m102.4, which neutralizes the virus by preventing its attachment to host cell receptors.
Animal studies have demonstrated significant protection when the antibody is administered early after exposure. Clinical trials and emergency-use protocols are currently evaluating the effectiveness and safety of this therapy in human patients.
3. Emerging Antiviral Agents
Several novel antiviral drugs are being studied for their potential activity against Nipah virus. Agents such as remdesivir have shown inhibitory effects on viral replication in laboratory and animal models. These drugs work by interfering with viral RNA polymerase enzymes that are essential for viral genome replication.
Although promising, these antiviral agents remain under investigation and are not yet widely available for routine clinical use. Continued research is essential to develop effective targeted therapies for Nipah virus infection.
D. Management of Neurological Complications
1. Treatment of Encephalitis
Encephalitis is one of the most severe complications of Nipah virus infection and involves inflammation of brain tissue due to viral invasion. Management requires close neurological monitoring, supportive care, and control of intracranial pressure. Patients may require admission to intensive care units for continuous neurological assessment.
The clinical importance of managing encephalitis lies in preventing irreversible neuronal damage and maintaining adequate cerebral perfusion. Early recognition of neurological deterioration significantly improves patient outcomes.
2. Control of Seizures
Seizures frequently occur in patients with Nipah virus encephalitis due to inflammation and disruption of neuronal activity. Anticonvulsant medications such as benzodiazepines, levetiracetam, or phenytoin are used to control seizure episodes and prevent recurrence.
Prompt seizure control is critical because prolonged seizures can cause additional brain injury, metabolic acidosis, and increased intracranial pressure. Continuous monitoring using electroencephalography may be required in severe cases.
3. Management of Cerebral Edema
Cerebral edema, or swelling of brain tissue, may occur during severe encephalitis and can lead to increased intracranial pressure. Treatment strategies include elevation of the head of the bed, osmotic therapy with agents such as mannitol, and controlled ventilation to regulate carbon dioxide levels.
Reducing intracranial pressure is essential for preventing brain herniation and maintaining adequate cerebral blood flow. Failure to manage cerebral edema effectively can result in rapid neurological deterioration and death.
E. Management of Respiratory Complications
1. Oxygen Therapy
Respiratory distress and hypoxemia are common in severe Nipah virus infection due to viral pneumonia and inflammation of lung tissue. Supplemental oxygen therapy is often required to maintain adequate oxygen saturation levels. Oxygen may be delivered through nasal cannula, face masks, or high-flow oxygen systems depending on the severity of respiratory compromise.
Maintaining adequate oxygenation is vital for preventing tissue hypoxia and organ dysfunction. Continuous monitoring of oxygen saturation and respiratory parameters helps guide treatment decisions.
2. Mechanical Ventilation
In cases of severe respiratory failure or acute respiratory distress syndrome, patients may require mechanical ventilation to support breathing. Ventilatory support ensures adequate gas exchange and reduces the workload on respiratory muscles.
Mechanical ventilation must be carefully managed using lung-protective strategies to prevent ventilator-induced lung injury. Intensive care monitoring is essential for optimizing respiratory function and preventing complications.
3. Prevention of Secondary Infections
Critically ill patients receiving prolonged respiratory support are at risk of secondary bacterial infections such as ventilator-associated pneumonia. Strict infection control practices, appropriate antibiotic therapy when indicated, and careful monitoring are necessary to prevent these complications.
Secondary infections can significantly worsen clinical outcomes and increase mortality. Early detection and treatment therefore play a crucial role in comprehensive patient management.
F. Management of Multiorgan Dysfunction
1. Cardiovascular Support
Severe Nipah virus infection can lead to hypotension, septic-like shock, and impaired circulation. Intravenous fluids and vasopressor medications such as norepinephrine may be required to maintain blood pressure and ensure adequate organ perfusion.
Cardiovascular stabilization is critical because prolonged hypotension can lead to irreversible damage to vital organs such as the brain, kidneys, and heart.
2. Renal Support
Acute kidney injury may occur due to systemic infection, dehydration, or multiorgan failure. Monitoring of urine output, serum creatinine, and electrolyte levels helps assess renal function. In severe cases, renal replacement therapy such as dialysis may be required.
Proper management of renal complications helps prevent accumulation of metabolic waste products and maintains electrolyte balance in critically ill patients.
3. Metabolic and Organ Support
Severe systemic infection can lead to metabolic disturbances such as acidosis, electrolyte imbalance, and hepatic dysfunction. Continuous laboratory monitoring and appropriate correction of metabolic abnormalities are essential components of treatment. Multiorgan support in intensive care settings significantly improves survival chances in patients with severe Nipah virus infection.
Currently, there is no universally approved specific antiviral therapy for Nipah virus infection, and treatment primarily focuses on intensive supportive care. Patients with suspected infection must be immediately isolated and managed in healthcare facilities capable of providing advanced monitoring and critical care support. Management includes maintenance of airway and breathing, oxygen therapy, and mechanical ventilation in cases of severe respiratory failure. Intravenous fluids, vasopressors, and careful hemodynamic monitoring are used to treat circulatory instability and shock. Anticonvulsant medications are administered to control seizures, and measures to reduce intracranial pressure may be required in severe encephalitis. Some antiviral agents such as ribavirin and investigational monoclonal antibodies have been studied, but their effectiveness remains under investigation. Early supportive management in an intensive care setting significantly improves survival and reduces complications.
Prevention and Control of Nipah Virus Infection
Prevention and control of Nipah virus infection represent the most important strategies for reducing disease burden because the infection is associated with high mortality and there is currently no universally available vaccine or definitive antiviral therapy. The virus is a zoonotic pathogen primarily maintained in nature by fruit bats of the genus Pteropus, which act as natural reservoirs and transmit the virus to humans either directly or through intermediate hosts such as pigs. Human-to-human transmission has also been documented during several outbreaks, particularly in healthcare settings and among family members caring for infected patients. Therefore, prevention requires a comprehensive approach that integrates animal health surveillance, environmental control, food safety practices, hospital infection control, community awareness, and strong public health systems. Effective preventive strategies aim to interrupt transmission pathways, detect outbreaks early, and protect both healthcare workers and the general population. 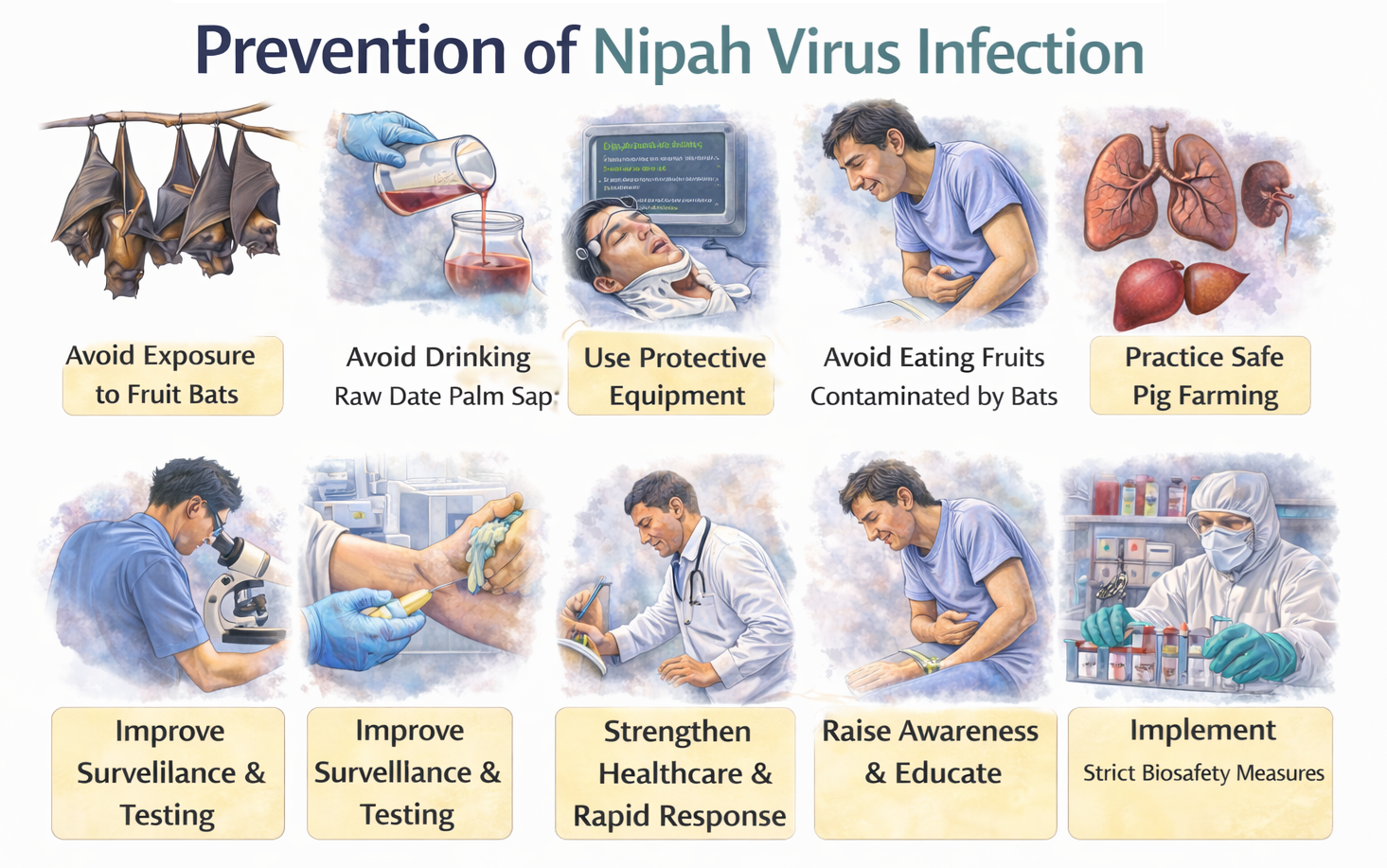
A. Prevention of Animal-to-Human Transmission
1. Avoidance of Consumption of Contaminated Fruits and Raw Palm Sap
Fruit bats, particularly species belonging to the Pteropus genus, are the natural reservoir hosts of the Nipah virus and can shed the virus in their saliva, urine, and feces. These secretions frequently contaminate fruits, fruit juices, and raw date palm sap, which are consumed by humans in many endemic regions. When bats feed on fruits or drink from sap collection pots, they may leave behind saliva or excreta containing the virus. Humans who consume these contaminated food products without proper washing, peeling, or processing may become infected.
From a clinical and epidemiological perspective, several outbreaks have been directly linked to the consumption of raw date palm sap or partially eaten fruits. Preventive measures therefore emphasize avoiding fruits that show evidence of bat bites, thoroughly washing fruits before consumption, and discouraging the consumption of raw palm sap collected in open containers. Public health authorities often promote the use of protective bamboo skirts or covers around sap collection pots to prevent bats from accessing them. These interventions have been shown to significantly reduce contamination and thereby decrease the risk of zoonotic transmission.
2. Prevention of Transmission from Domestic Animals
Domestic animals can serve as intermediate or amplifying hosts for the Nipah virus, particularly pigs. During the first recognized outbreak of the disease, large numbers of pig farmers and farm workers were infected after direct contact with infected pigs. The virus can cause respiratory and neurological illness in pigs, and infected animals may shed the virus through respiratory secretions, saliva, and urine, facilitating transmission to humans who handle them.
Preventive strategies therefore involve regular veterinary surveillance and monitoring of livestock populations for signs of unusual illness, particularly respiratory disease or neurological abnormalities. Farmers and animal handlers should use protective measures such as gloves, masks, and protective clothing when dealing with sick animals. In suspected outbreaks among animals, quarantine measures and sometimes culling of infected livestock may be necessary to prevent further spread. Veterinary authorities must collaborate closely with public health agencies to ensure early detection and rapid response to potential zoonotic transmission events.
3. Limiting Human Contact with Wildlife Reservoirs
Direct interaction with wildlife reservoirs such as fruit bats increases the risk of exposure to the Nipah virus. Activities including hunting, handling injured bats, disturbing bat colonies, or consuming bushmeat may increase opportunities for viral transmission. People living near bat habitats may also encounter bats in orchards or agricultural areas where bats feed on cultivated fruits.
Public health education programs encourage communities to avoid direct contact with bats and other potentially infected wildlife. Environmental strategies may include protecting fruit orchards using nets, reducing bat access to human food sources, and discouraging activities that bring humans into close proximity with bat populations. These interventions are essential in rural areas where human-wildlife interactions are frequent and may facilitate zoonotic spillover.
B. Prevention of Human-to-Human Transmission
1. Early Identification and Isolation of Suspected Cases
Human-to-human transmission of Nipah virus infection has been documented in several outbreaks, particularly through close contact with infected individuals or exposure to respiratory secretions and body fluids. Early identification of suspected cases is therefore critical in preventing secondary transmission. Patients presenting with acute febrile illness accompanied by neurological symptoms such as headache, confusion, seizures, or altered consciousness should be carefully evaluated, especially in regions where Nipah outbreaks have previously occurred.
Once a suspected case is identified, immediate isolation in a designated healthcare facility is necessary until laboratory confirmation is obtained. Isolation helps prevent exposure to other patients, healthcare workers, and visitors. Early isolation has been shown to significantly reduce transmission within healthcare facilities and communities, making it one of the most effective outbreak control measures.
2. Infection Control Practices in Healthcare Settings
Healthcare settings represent high-risk environments for the transmission of Nipah virus because healthcare workers often come into close contact with infected patients and their bodily fluids. Strict infection prevention and control measures must therefore be implemented when managing suspected or confirmed cases. Healthcare personnel should use appropriate personal protective equipment, including gloves, gowns, masks or respirators, eye protection, and face shields.
In addition to protective equipment, proper hand hygiene practices are essential before and after patient contact. Medical procedures that generate aerosols, such as intubation, suctioning, or mechanical ventilation, require additional precautions to minimize airborne transmission. Dedicated isolation wards, trained infection control teams, and proper environmental disinfection protocols further enhance safety within healthcare facilities. These measures protect healthcare workers and prevent hospital-based outbreaks.
3. Contact Tracing and Monitoring of Exposed Individuals
During an outbreak, individuals who have had close contact with infected patients must be identified and monitored for signs of illness. Contact tracing involves identifying family members, caregivers, healthcare workers, and other individuals who may have been exposed to the virus through close interaction with the infected patient. These contacts are typically monitored for symptoms during the incubation period, which usually ranges from 4 to 14 days but may occasionally extend longer.
Monitoring may include regular health checks, temperature monitoring, and prompt medical evaluation if symptoms develop. In some situations, quarantine measures may be implemented for high-risk contacts to prevent potential spread within the community. Effective contact tracing and monitoring are essential components of outbreak control and can significantly reduce the spread of infection.
C. Community Awareness and Public Health Education
1. Public Health Education Campaigns
Community awareness is one of the most effective tools for preventing Nipah virus outbreaks. Many infections occur because individuals are unaware of the transmission routes or preventive measures. Public health education campaigns aim to inform communities about the natural reservoirs of the virus, modes of transmission, early symptoms of infection, and steps that can be taken to reduce exposure.
Educational programs may involve mass media campaigns, community meetings, training sessions for healthcare workers, and distribution of informational materials. By increasing public knowledge about the disease, these programs encourage early reporting of suspected cases and adoption of preventive behaviors, which are essential for controlling outbreaks.
2. Promotion of Personal Hygiene Practices
Basic hygiene measures can significantly reduce the risk of infection. Regular handwashing with soap and water, use of alcohol-based hand sanitizers, and avoiding direct contact with bodily fluids of infected individuals are essential preventive practices. Individuals caring for sick family members should use protective measures such as gloves and masks whenever possible.
In healthcare and community settings alike, hygiene practices serve as a primary barrier against infectious disease transmission. Reinforcing these practices through education and public health campaigns can greatly reduce the spread of Nipah virus and other communicable diseases.
3. Addressing Cultural and Behavioral Risk Factors
In some regions, traditional practices such as consumption of fresh date palm sap or close interaction with domestic animals are deeply embedded in cultural and economic activities. While these practices may increase the risk of exposure to Nipah virus, prevention strategies must be designed in a culturally sensitive manner.
Public health authorities often work with community leaders to promote safer alternatives while respecting cultural traditions. For example, covering date palm sap collection pots to prevent bat contamination allows communities to continue traditional practices while reducing infection risk. Such culturally appropriate interventions increase community acceptance and improve the effectiveness of preventive measures.
D. Surveillance, Early Detection, and Public Health Response
1. Epidemiological Surveillance Systems
Surveillance systems play a crucial role in detecting Nipah virus outbreaks at an early stage. Public health authorities must monitor unusual clusters of severe respiratory illness or encephalitis, particularly in regions with known Nipah virus activity. Early detection enables rapid implementation of containment measures such as patient isolation, contact tracing, and community awareness campaigns.
Effective surveillance requires collaboration between hospitals, laboratories, veterinary agencies, and public health departments. Data collected through surveillance programs help identify patterns of disease transmission, assess risk factors, and guide preventive strategies.
2. Strengthening Laboratory Diagnostic Capacity
Accurate laboratory diagnosis is essential for confirming suspected cases and guiding outbreak response. Diagnostic techniques such as reverse transcription polymerase chain reaction detect viral genetic material in patient samples, while serological tests identify antibodies produced in response to infection.
Strengthening laboratory infrastructure ensures that suspected cases can be rapidly confirmed, allowing healthcare providers and public health authorities to implement appropriate control measures. Reliable diagnostic capabilities also help distinguish Nipah virus infection from other diseases with similar clinical presentations, such as viral encephalitis caused by other pathogens.
3. International Collaboration and Information Sharing
Because Nipah virus outbreaks can pose global health threats, international collaboration is essential for effective prevention and control. Organizations such as the World Health Organization coordinate global surveillance, provide technical guidance, and support countries in responding to outbreaks.
International information sharing enables rapid dissemination of epidemiological data, research findings, and best practices for disease management. Collaborative research efforts also contribute to the development of vaccines, antiviral therapies, and improved diagnostic tools.
E. Research, Vaccine Development, and Future Preventive Strategies
1. Development of Vaccines Against Nipah Virus
Currently, there is no widely approved vaccine available for preventing Nipah virus infection in humans. However, several vaccine candidates are under development using advanced biotechnology platforms such as viral vector vaccines, recombinant protein vaccines, and nucleic acid-based vaccines. These experimental vaccines aim to stimulate protective immune responses against viral surface glycoproteins responsible for host cell entry.
Preclinical studies in animal models have demonstrated promising levels of immunity and protection. Ongoing research and clinical trials are necessary to determine the safety, efficacy, and long-term protection offered by these vaccine candidates before they can be widely implemented in public health programs.
2. Development of Therapeutic Antibodies for Prophylaxis
Monoclonal antibody therapies that neutralize Nipah virus are being investigated not only for treatment but also for post-exposure prophylaxis. These antibodies work by binding to viral surface proteins and preventing the virus from attaching to and entering host cells.
Such therapies may provide immediate passive immunity to individuals exposed to the virus during outbreaks, particularly healthcare workers or family members caring for infected patients. If proven effective in clinical trials, antibody-based interventions may become an important preventive tool during outbreak situations.
3. Strengthening Global Preparedness for Emerging Zoonotic Diseases
Nipah virus is classified among priority emerging pathogens because of its high mortality rate, potential for human-to-human transmission, and lack of widely available vaccines or treatments. Strengthening global preparedness involves improving disease surveillance systems, investing in research and development, training healthcare professionals, and establishing rapid outbreak response teams.
Preparedness efforts also include strengthening healthcare infrastructure, enhancing laboratory capacity, and promoting international collaboration. These measures not only help control Nipah virus outbreaks but also improve the global capacity to respond to other emerging infectious diseases.
Prevention of Nipah virus infection focuses on reducing exposure to infected animals, contaminated food sources, and infected individuals. Public health measures include avoiding consumption of raw date palm sap or fruits that may have been contaminated by bats, maintaining proper food hygiene, and preventing bats from accessing food collection areas. Farmers and animal handlers should implement protective measures when handling livestock and avoid contact with sick animals. During outbreaks, strict infection-control practices in healthcare settings are essential, including the use of personal protective equipment, proper isolation of patients, and careful handling of bodily fluids. Community awareness programs and surveillance systems play a crucial role in early detection and containment of outbreaks. Strengthening coordination between human health, veterinary, and environmental sectors is critical for preventing future outbreaks and controlling the spread of Nipah virus infection.
Common FAQs on Nipah virus infection
- What is Nipah virus infection?
Nipah virus infection is a severe zoonotic disease caused by a virus belonging to the Henipavirus genus. It primarily affects the respiratory and nervous systems. Humans become infected through contact with infected animals, contaminated food, or infected individuals. The disease often progresses rapidly to encephalitis and respiratory failure, and it has a high mortality rate, making it an important global public health concern.
- What are the common symptoms of Nipah virus infection?
The symptoms of Nipah virus infection usually begin with high fever, headache, muscle pain, fatigue, and sore throat. As the infection progresses, patients may develop vomiting, dizziness, and respiratory symptoms such as cough and breathing difficulty. In severe cases, the virus affects the brain, leading to confusion, seizures, neurological deficits, and coma. Rapid progression of neurological symptoms is a characteristic feature of the disease.
- How does Nipah virus spread to humans?
Nipah virus spreads to humans primarily through zoonotic transmission from infected animals, particularly fruit bats or pigs. Humans can become infected by consuming food contaminated with bat saliva or urine, such as raw date palm sap. Person-to-person transmission can also occur through close contact with respiratory secretions, body fluids, or contaminated surfaces of infected individuals, especially in healthcare settings without adequate infection control measures.
- Which animals act as reservoirs for Nipah virus?
Fruit bats belonging to the genus Pteropus are the natural reservoirs of the virus. These bats carry the virus without developing disease and shed it through saliva, urine, and partially eaten fruits. Domestic animals such as pigs may act as intermediate hosts and amplify the virus before transmitting it to humans. The interaction between bats, livestock, and humans increases the risk of zoonotic spillover events.
- Who is at higher risk of Nipah virus infection?
Individuals living in regions where Nipah virus outbreaks occur have a higher risk of infection. Farmers, animal handlers, veterinarians, and slaughterhouse workers may be exposed through contact with infected animals. Healthcare workers and family members caring for infected patients are also at risk due to close contact with body fluids or respiratory secretions. Consumption of contaminated food products further increases exposure risk in endemic areas.
- How is Nipah virus infection diagnosed?
Diagnosis requires laboratory confirmation combined with clinical and epidemiological assessment. The most reliable diagnostic method is real-time reverse transcription polymerase chain reaction (RT-PCR), which detects viral genetic material in respiratory samples, blood, cerebrospinal fluid, or urine. Serological tests such as IgM and IgG ELISA can detect antibodies produced against the virus. Imaging studies like MRI may support diagnosis by revealing characteristic brain lesions.
- Why is Nipah virus considered a highly dangerous infection?
Nipah virus is considered dangerous because it causes severe neurological disease and respiratory complications with a high case-fatality rate. The virus can spread through zoonotic transmission and human-to-human contact, particularly in healthcare environments. Rapid progression of encephalitis and respiratory failure often leads to death. Additionally, the absence of a widely approved vaccine or specific antiviral therapy increases the threat posed by the infection.
- What complications can occur in Nipah virus infection?
Complications arise due to systemic viral invasion and vascular injury. The most serious complication is acute encephalitis, which causes seizures, coma, and long-term neurological damage. Respiratory complications such as pneumonitis and acute respiratory distress syndrome can lead to severe hypoxemia. Some survivors may experience persistent neurological deficits, personality changes, or recurrent encephalitis months after recovery, highlighting the long-term impact of the infection.
- Is there a specific treatment for Nipah virus infection?
Currently, there is no universally approved antiviral treatment specifically for Nipah virus infection. Management focuses on supportive medical care aimed at maintaining vital functions. Patients often require hospitalization in intensive care units where they receive oxygen therapy, mechanical ventilation, intravenous fluids, and medications to control seizures. Early supportive care and careful monitoring are essential to reduce complications and improve survival outcomes.
- How can Nipah virus infection be prevented?
Prevention involves minimizing contact with infected animals, contaminated food sources, and infected individuals. Avoiding consumption of raw date palm sap or fruits contaminated by bats is an important preventive measure in endemic regions. Maintaining strict hygiene practices, using protective equipment in healthcare settings, and implementing isolation protocols for suspected cases help reduce transmission. Public health surveillance and community awareness programs also play vital roles.
- What organs are primarily affected by Nipah virus?
Nipah virus mainly affects the central nervous system and the respiratory system. Viral invasion of the brain leads to inflammation known as encephalitis, which causes neurological symptoms such as confusion, seizures, and coma. The lungs may develop severe inflammation and pneumonitis, resulting in respiratory distress and oxygen deficiency. In advanced stages, the infection may also involve other organs, causing systemic complications.
- Can Nipah virus spread from person to person?
Yes, person-to-person transmission of Nipah virus has been documented during several outbreaks. The virus can spread through close contact with respiratory droplets, saliva, urine, or other body fluids of infected individuals. Healthcare workers and family members providing care are particularly vulnerable if appropriate protective measures are not used. Strict infection control procedures are therefore critical to prevent secondary transmission during outbreaks.
- What is the mortality rate of Nipah virus infection?
The mortality rate of Nipah virus infection is extremely high compared with many other viral diseases. Reported case-fatality rates typically range from about 40 percent to 75 percent, depending on healthcare infrastructure, early diagnosis, and availability of supportive treatment. Severe neurological involvement and respiratory failure significantly increase the risk of death. Early detection and intensive medical care are essential to improve survival chances.
- Can survivors of Nipah virus infection have long-term effects?
Yes, some individuals who survive Nipah virus infection may experience long-term neurological complications. These may include persistent seizures, memory impairment, personality changes, and reduced cognitive function. In rare cases, survivors develop relapsing or late-onset encephalitis months or years after the initial illness. These chronic neurological effects highlight the need for long-term follow-up and neurological monitoring of recovered patients.
- Why is surveillance important in controlling Nipah virus outbreaks?
Surveillance plays a critical role in detecting early cases and preventing widespread outbreaks. Monitoring animal reservoirs, particularly fruit bats and livestock, helps identify potential transmission sources. Early identification of human cases allows rapid isolation, contact tracing, and implementation of infection control measures. Strong surveillance systems also support public health preparedness and facilitate coordinated responses to emerging infectious disease threats like Nipah virus.
Bibliography on Nipah Virus Infection
- Henipavirus: Ecology, Molecular Virology, and Pathogenesis – Editors: B. Lee and P. A. Rota, Publisher: Springer.
- Oxford Textbook of Medicine – Editors: J. Firth, C. Conlon, and T. Cox, Publisher: Oxford University Press.
- Mandell, Douglas, and Bennett’s Principles and Practice of Infectious Diseases – Editors: J. E. Bennett, R. Dolin, and M. J. Blaser, Publisher: Elsevier.
- Harrison’s Principles of Internal Medicine – Editors: J. L. Jameson, A. S. Fauci, D. L. Kasper, S. L. Hauser, and J. Loscalzo, Publisher: McGraw-Hill Education.
- Medical Microbiology – Authors: P. R. Murray, K. S. Rosenthal, and M. A. Pfaller, Publisher: Elsevier.
- Sherris Medical Microbiology – Authors: K. J. Ryan and C. G. Ray, Publisher: McGraw-Hill Education.
- Nipah Virus: Methods and Protocols – Editor: A. N. Freiberg, Publisher: Humana Press, Springer Nature.
- Manson’s Tropical Diseases – Authors: G. C. Cook and A. I. Zumla, Publisher: Elsevier.
- Principles of Virology – Authors: S. J. Flint, V. R. Racaniello, G. F. Rall, A. M. Skalka, and L. W. Enquist, Publisher: ASM Press.
- Desk Encyclopedia of Human and Medical Virology – Editors: B. W. J. Mahy and M. H. V. Van Regenmortel, Publisher: Academic Press.
- Infectious Diseases – Editors: J. Cohen, W. G. Powderly, and S. M. Opal, Publisher: Elsevier.
- Medical Microbiology – Editor: S. Baron, Publisher: University of Texas Medical Branch.
- Nipah Virus Infection – Authors: B. S. P. Ang, T. C. C. Lim, and L. Wang, Journal: Journal of Clinical Microbiology.
- Nipah Virus Infection: A Review – Authors: Aditi and M. Shariff, Journal: Epidemiology and Infection.
- Recurrent Zoonotic Transmission of Nipah Virus into Humans, Bangladesh, 2001–2007 – Authors: S. P. Luby et al., Journal: Emerging Infectious Diseases.